

Description
Klinefelter syndrome, also called 47,XXY, is a chromosomal condition that affects male development. The signs and symptoms of Klinefelter syndrome vary. In some cases, the features are so mild that the condition is not diagnosed until puberty or adulthood. Researchers believe that up to 65 percent of people with Klinefelter syndrome are never diagnosed.
Individuals with Klinefelter syndrome typically have small testes that produce a reduced amount of testosterone (primary testicular insufficiency). Testosterone is the hormone that directs male sexual development before birth and during puberty. A small percentage of affected individuals are born with undescended testes (cryptorchidism). Without treatment, the shortage of testosterone can lead to delayed or incomplete puberty, breast enlargement (gynecomastia), decreased muscle mass, decreased bone density, a reduced amount of facial and body hair, and fatigue. Klinefelter syndrome can make it difficult for people with this condition to have biological children (a condition called infertility), but up to half of people with Klinefelter syndrome may be able to have children using assisted reproductive technologies..
The other physical changes associated with Klinefelter syndrome are usually subtle. Most commonly, affected individuals are taller than average and 2 to 3 inches taller than would be expected for their family. Other features can include curved pinky fingers (fifth finger clinodactyly ), flat feet (pes planus
), flat feet (pes planus ), and, less commonly, abnormal fusion of certain bones in the forearm (radioulnar synostosis).
), and, less commonly, abnormal fusion of certain bones in the forearm (radioulnar synostosis).
Children with Klinefelter syndrome may have low muscle tone (hypotonia), difficulty coordinating movements, and mild delays of certain developmental skills, such as rolling over or walking. Affected children have an increased risk of mild delays in speech and language development. People with Klinefelter syndrome tend to have better receptive language skills (the ability to understand speech) than expressive language skills (vocabulary and the production of speech) and may have difficulty communicating and expressing themselves. Affected individuals have an increased risk for learning disabilities, most commonly problems with reading (dyslexia) and written expression. People with Klinefelter syndrome very rarely have intellectual disabilities.
Individuals with Klinefelter syndrome may have have anxiety, depression, impaired social skills, or behavioral differences, such as emotional immaturity during childhood or difficulty with frustration. Affected individuals also have an increased risk for attention-deficit/hyperactivity disorder (ADHD), though they tend to have problems with attention and distractability rather than hyperactivity. People with Klinefelter syndrome are more likely than those without Klinefelter syndrome to have autism spectrum disorder, which is a developmental disorder that affects communication and social interaction.
People with Klinefelter syndrome have an increased risk of developing metabolic syndrome, which is a group of conditions that include high blood glucose levels during prolonged periods without food (fasting), high blood pressure (hypertension), increased belly fat, and high levels of fats (lipids) such as cholesterol and triglycerides in the blood. Compared with unaffected people, adults with Klinefelter syndrome also have an increased risk of developing involuntary trembling (tremors) in their arms or hands, breast cancer (if gynecomastia develops), thinning and weakening of the bones (osteoporosis), and autoimmune disorders such as systemic lupus erythematosus and rheumatoid arthritis. Autoimmune disorders are a large group of conditions that occur when the immune system attacks the body's own tissues and organs.
Frequency
Klinefelter syndrome affects about 1 in 650 male newborns. It is the most common sex chromosome disorder, which is a group of conditions caused by changes in the number of sex chromosomes (the X chromosome and the Y chromosome).
(the X chromosome and the Y chromosome).
Causes
Klinefelter syndrome is a sex chromosome disorder that results from the presence of an extra X chromosome in cells. People typically have 46 chromosomes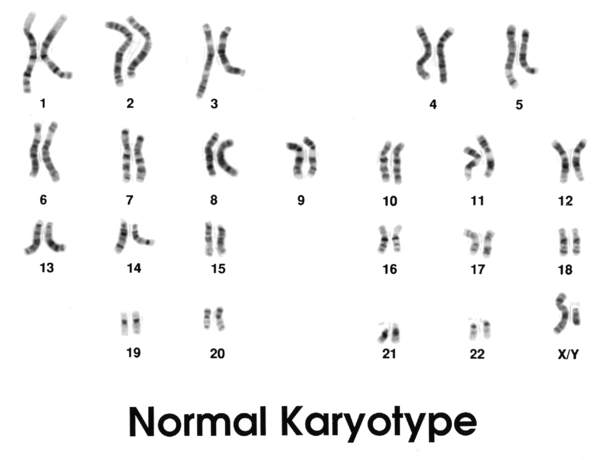 in each cell, two of which are the sex chromosomes. Females typically have two X chromosomes (46,XX), and males typically have one X and one Y chromosome (46,XY). Most often, people with Klinefelter syndrome have the usual X and Y chromosomes, and one extra X chromosome, for a total of 47 chromosomes (47,XXY).
in each cell, two of which are the sex chromosomes. Females typically have two X chromosomes (46,XX), and males typically have one X and one Y chromosome (46,XY). Most often, people with Klinefelter syndrome have the usual X and Y chromosomes, and one extra X chromosome, for a total of 47 chromosomes (47,XXY).
Individuals with Klinefelter syndrome have an extra copy of multiple genes on the X chromosome. The activity of these extra genes may disrupt many aspects of development and are responsible for the common signs and symptoms of Klinefelter syndrome. Researchers are working to determine which genes contribute to the specific developmental and physical differences that can occur in people with Klinefelter syndrome.
Some people with features of Klinefelter syndrome have an extra X chromosome in only some of their cells, while the other cells have one X and one Y chromosome. Rarely, some cells may have additional chromosome abnormalities. In these individuals, the condition is described as mosaic Klinefelter syndrome (46,XY/47,XXY). It is thought that approximately 10 percent of individuals with Klinefelter syndrome have the mosaic form. People with mosaic Klinefelter syndrome may have milder signs and symptoms than those with the extra X chromosome in all of their cells, depending on what proportion of cells have the additional chromosome.
Some conditions that are caused by the presence of more than one extra sex chromosome in each cell are described as variants of Klinefelter syndrome. These conditions include 48,XXXY syndrome, 48,XXYY syndrome, and 49,XXXXY syndrome. Like Klinefelter syndrome, these conditions affect male sexual development and can be associated with learning disabilities and problems with speech and language development. However, the features of these disorders tend to be more severe than those of Klinefelter syndrome and affect more parts of the body. As doctors and researchers have learned more about the differences between these sex chromosome disorders, they have started to classify them as separate conditions.
Inheritance
Klinefelter syndrome is not inherited; the addition of an extra X chromosome occurs during the formation of reproductive cells (eggs or sperm) in one of an affected person's parents. During cell division, an error called nondisjunction prevents X chromosomes from being distributed normally among reproductive cells as they form. Typically, as cells divide, each egg cell gets a single X chromosome, and each sperm cell gets either an X chromosome or a Y chromosome. However, because of nondisjunction, an egg cell or a sperm cell can also end up with an extra copy of the X chromosome.
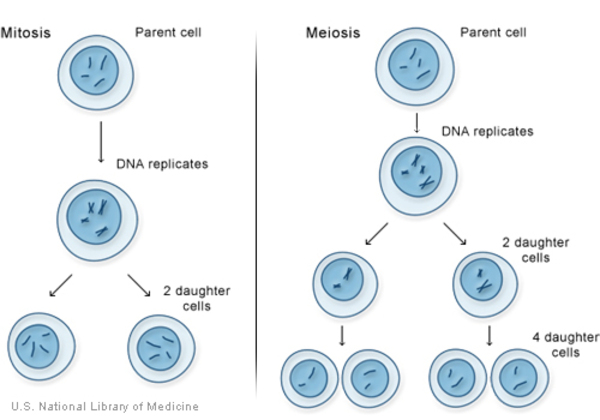
If an egg cell with an extra X chromosome (XX) is fertilized by a sperm cell with one Y chromosome, the resulting child will have Klinefelter syndrome. Similarly, if a sperm cell with both an X chromosome and a Y chromosome (XY) fertilizes an egg cell with a single X chromosome, the resulting child will have Klinefelter syndrome.
Mosaic Klinefelter syndrome (46,XY/47,XXY) is also not inherited. It occurs as a random error during cell division early in fetal development. As a result, some of the body's cells have the usual one X chromosome and one Y chromosome (46,XY), and other cells have an extra copy of the X chromosome (47,XXY).
Other Names for This Condition
- 47,XXY syndrome
- Klinefelter syndrome (KS)
- Klinefelter's syndrome
- XXY syndrome
- XXY trisomy
Additional Information & Resources
Genetic Testing Information
Patient Support and Advocacy Resources
Clinical Trials
Scientific Articles on PubMed
References
- Boada R, Janusz J, Hutaff-Lee C, Tartaglia N. The cognitive phenotype in Klinefelter syndrome: a review of the literature including genetic and hormonal factors. Dev Disabil Res Rev. 2009;15(4):284-94. doi: 10.1002/ddrr.83. Citation on PubMed or Free article on PubMed Central
- Davis S, Howell S, Wilson R, Tanda T, Ross J, Zeitler P, Tartaglia N. Advances in the Interdisciplinary Care of Children with Klinefelter Syndrome. Adv Pediatr. 2016 Aug;63(1):15-46. doi: 10.1016/j.yapd.2016.04.020. No abstract available. Citation on PubMed or Free article on PubMed Central
- Fruhmesser A, Kotzot D. Chromosomal variants in klinefelter syndrome. Sex Dev. 2011;5(3):109-23. doi: 10.1159/000327324. Epub 2011 Apr 29. Citation on PubMed
- Giltay JC, Maiburg MC. Klinefelter syndrome: clinical and molecular aspects. Expert Rev Mol Diagn. 2010 Sep;10(6):765-76. doi: 10.1586/erm.10.63. Citation on PubMed
- Groth KA, Skakkebaek A, Host C, Gravholt CH, Bojesen A. Clinical review: Klinefelter syndrome--a clinical update. J Clin Endocrinol Metab. 2013 Jan;98(1):20-30. doi: 10.1210/jc.2012-2382. Epub 2012 Nov 1. Citation on PubMed
- Herlihy AS, Gillam L. Thinking outside the square: considering gender in Klinefelter syndrome and 47, XXY. Int J Androl. 2011 Oct;34(5 Pt 2):e348-9. doi: 10.1111/j.1365-2605.2010.01132.x. Epub 2011 Mar 31. No abstract available. Citation on PubMed
- Nieschlag E, Ferlin A, Gravholt CH, Gromoll J, Kohler B, Lejeune H, Rogol AD, Wistuba J. The Klinefelter syndrome: current management and research challenges. Andrology. 2016 May;4(3):545-9. doi: 10.1111/andr.12208. No abstract available. Citation on PubMed
- Nieschlag E. Klinefelter syndrome: the commonest form of hypogonadism, but often overlooked or untreated. Dtsch Arztebl Int. 2013 May;110(20):347-53. doi: 10.3238/arztebl.2013.0347. Epub 2013 May 17. Citation on PubMed or Free article on PubMed Central
- Radicioni AF, Ferlin A, Balercia G, Pasquali D, Vignozzi L, Maggi M, Foresta C, Lenzi A. Consensus statement on diagnosis and clinical management of Klinefelter syndrome. J Endocrinol Invest. 2010 Dec;33(11):839-50. doi: 10.1007/BF03350351. Citation on PubMed
- Sokol RZ. It's not all about the testes: medical issues in Klinefelter patients. Fertil Steril. 2012 Aug;98(2):261-5. doi: 10.1016/j.fertnstert.2012.05.026. Epub 2012 Jun 15. Citation on PubMed
- Swerdlow AJ, Schoemaker MJ, Higgins CD, Wright AF, Jacobs PA; UK Clinical Cytogenetics Group. Cancer incidence and mortality in men with Klinefelter syndrome: a cohort study. J Natl Cancer Inst. 2005 Aug 17;97(16):1204-10. doi: 10.1093/jnci/dji240. Citation on PubMed
- Tartaglia N, Ayari N, Howell S, D'Epagnier C, Zeitler P. 48,XXYY, 48,XXXY and 49,XXXXY syndromes: not just variants of Klinefelter syndrome. Acta Paediatr. 2011 Jun;100(6):851-60. doi: 10.1111/j.1651-2227.2011.02235.x. Epub 2011 Apr 8. Citation on PubMed or Free article on PubMed Central
- Tartaglia N, Cordeiro L, Howell S, Wilson R, Janusz J. The spectrum of the behavioral phenotype in boys and adolescents 47,XXY (Klinefelter syndrome). Pediatr Endocrinol Rev. 2010 Dec;8 Suppl 1(0 1):151-9. Citation on PubMed or Free article on PubMed Central
- Tartaglia NR, Wilson R, Miller JS, Rafalko J, Cordeiro L, Davis S, Hessl D, Ross J. Autism Spectrum Disorder in Males with Sex Chromosome Aneuploidy: XXY/Klinefelter Syndrome, XYY, and XXYY. J Dev Behav Pediatr. 2017 Apr;38(3):197-207. doi: 10.1097/DBP.0000000000000429. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.