

Description
Attention-deficit/hyperactivity disorder (ADHD) is a behavioral disorder that typically begins in childhood and is characterized by a short attention span (inattention), an inability to be calm and stay still (hyperactivity), and poor impulse control (impulsivity). Some people with ADHD have problems with only inattention or with hyperactivity and impulsivity, but most have problems related to all three features.
In people with ADHD, the characteristic behaviors are frequent and severe enough to interfere with the activities of daily living such as school, work, and relationships with others. Because of an inability to stay focused on tasks, people with inattention may be easily distracted, forgetful, avoid tasks that require sustained attention, have difficulty organizing tasks, or frequently lose items.
Hyperactivity is usually shown by frequent movement. Individuals with this feature often fidget or tap their foot when seated, leave their seat when it is inappropriate to do so (such as in the classroom), or talk a lot and interrupt others.
Impulsivity can result in hasty actions without thought for the consequences. Individuals with poor impulse control may have difficulty waiting for their turn, deferring to others, or considering their actions before acting.
More than two-thirds of all individuals with ADHD have additional conditions, including insomnia, mood or anxiety disorders, learning disorders, or substance use disorders. Affected individuals may also have autism spectrum disorder, which is characterized by impaired communication and social interaction, or Tourette syndrome, which is a disorder characterized by repetitive and involuntary movements or noises called tics.
In most affected individuals, ADHD continues throughout life, but in about one-third of individuals, signs and symptoms of ADHD go away by adulthood.
Frequency
Worldwide, ADHD affects approximately 5 percent of children and 3 percent of adults.
Causes
Changes in dozens of genes have been associated with ADHD. Many gene variations, most of which have not been identified, are thought to affect the risk of developing ADHD. Because they are common in many populations worldwide, not all people with these gene variations will have the condition. Many of the gene variations have only a small effect, and most people with ADHD are thought to have numerous associated gene variations. These variations also combine with environmental risk factors to determine an individual's risk of developing this complex condition. Environmental risk factors that may contribute to the development of ADHD include complications during pregnancy and delivery and exposure to heavy metals such as lead. It is unclear how genetic and environmental factors influence each other to contribute to ADHD.
Less commonly, ADHD is caused by rare gene mutations or chromosome abnormalities. In these instances, ADHD is usually one of several features of a syndrome that affects multiple parts of the body. In most individuals with ADHD caused by rare gene mutations, a mutation in a single gene is enough to cause the disorder.
The genes associated with ADHD are thought to be involved in the development of the brain. The various proteins produced from these genes affect multiple aspects of brain development, including production, growth, or organization of nerve cells (neurons). Other genes associated with ADHD provide instructions for proteins that are important for communication between neurons. Some of these proteins help produce or control the chemicals that relay communication signals between neurons (neurotransmitters). Other proteins have roles at the connections between neurons (synapses) where this communication takes place.

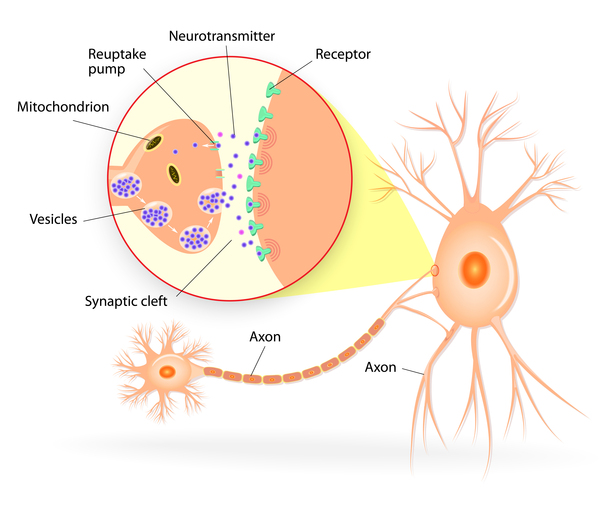

The specific ways that changes in associated genes are involved in the development of ADHD are unknown. Research has found that people with ADHD often have low levels of the neurotransmitter dopamine, which has many important functions, including having complex roles in thought (cognition), motivation, behavior, and control of movement. Certain layers of the brain may also develop somewhat differently than usual in people with ADHD.
Inheritance
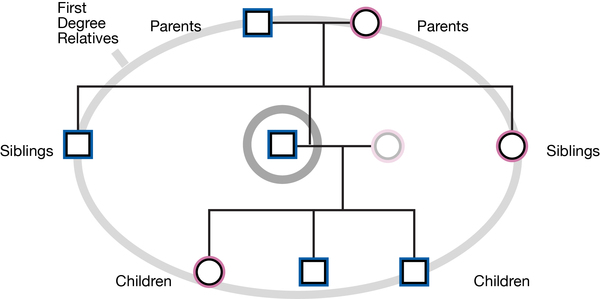
ADHD has a tendency to run in families, but the inheritance pattern is usually unknown. Overall, the risk of developing this condition is about nine times greater for first-degree relatives of people with the condition (such as siblings or children) as compared to the general public. People with genetic changes associated with ADHD generally inherit an increased risk of developing the condition, rather than the condition itself. When ADHD is a feature of another genetic syndrome, it can be passed on according to the inheritance pattern of that syndrome.
Other Names for This Condition
- ADD
- ADDH
- ADHD
- Attention deficit
- Attention deficit disorder
- Attention deficit disorder of childhood with hyperactivity
- Attention deficit disorder with hyperactivity
- Attention deficit disorder with hyperactivity syndrome
- Attention deficit hyperactivity disorder
- Hyperkinetic disorder
- Hyperkinetic syndrome
Additional Information & Resources
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Belanger SA, Andrews D, Gray C, Korczak D. ADHD in children and youth: Part 1-Etiology, diagnosis, and comorbidity. Paediatr Child Health. 2018 Nov;23(7):447-453. doi: 10.1093/pch/pxy109. Epub 2018 Oct 24. Citation on PubMed or Free article on PubMed Central
- Demontis D, Walters RK, Martin J, Mattheisen M, Als TD, Agerbo E, Baldursson G, Belliveau R, Bybjerg-Grauholm J, Baekvad-Hansen M, Cerrato F, Chambert K, Churchhouse C, Dumont A, Eriksson N, Gandal M, Goldstein JI, Grasby KL, Grove J, Gudmundsson OO, Hansen CS, Hauberg ME, Hollegaard MV, Howrigan DP, Huang H, Maller JB, Martin AR, Martin NG, Moran J, Pallesen J, Palmer DS, Pedersen CB, Pedersen MG, Poterba T, Poulsen JB, Ripke S, Robinson EB, Satterstrom FK, Stefansson H, Stevens C, Turley P, Walters GB, Won H, Wright MJ; ADHD Working Group of the Psychiatric Genomics Consortium (PGC); Early Lifecourse & Genetic Epidemiology (EAGLE) Consortium; 23andMe Research Team; Andreassen OA, Asherson P, Burton CL, Boomsma DI, Cormand B, Dalsgaard S, Franke B, Gelernter J, Geschwind D, Hakonarson H, Haavik J, Kranzler HR, Kuntsi J, Langley K, Lesch KP, Middeldorp C, Reif A, Rohde LA, Roussos P, Schachar R, Sklar P, Sonuga-Barke EJS, Sullivan PF, Thapar A, Tung JY, Waldman ID, Medland SE, Stefansson K, Nordentoft M, Hougaard DM, Werge T, Mors O, Mortensen PB, Daly MJ, Faraone SV, Borglum AD, Neale BM. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat Genet. 2019 Jan;51(1):63-75. doi: 10.1038/s41588-018-0269-7. Epub 2018 Nov 26. Citation on PubMed or Free article on PubMed Central
- Faraone SV, Larsson H. Genetics of attention deficit hyperactivity disorder. Mol Psychiatry. 2019 Apr;24(4):562-575. doi: 10.1038/s41380-018-0070-0. Epub 2018 Jun 11. Citation on PubMed or Free article on PubMed Central
- Feldman ME, Charach A, Belanger SA. ADHD in children and youth: Part 2-Treatment. Paediatr Child Health. 2018 Nov;23(7):462-472. doi: 10.1093/pch/pxy113. Epub 2018 Oct 24. Citation on PubMed or Free article on PubMed Central
- Gorman DA, Gardner DM, Murphy AL, Feldman M, Belanger SA, Steele MM, Boylan K, Cochrane-Brink K, Goldade R, Soper PR, Ustina J, Pringsheim T. Canadian guidelines on pharmacotherapy for disruptive and aggressive behaviour in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, or conduct disorder. Can J Psychiatry. 2015 Feb;60(2):62-76. doi: 10.1177/070674371506000204. Citation on PubMed or Free article on PubMed Central
- Larsson H, Anckarsater H, Rastam M, Chang Z, Lichtenstein P. Childhood attention-deficit hyperactivity disorder as an extreme of a continuous trait: a quantitative genetic study of 8,500 twin pairs. J Child Psychol Psychiatry. 2012 Jan;53(1):73-80. doi: 10.1111/j.1469-7610.2011.02467.x. Epub 2011 Sep 16. Citation on PubMed
- Subcommittee on Attention-Deficit/Hyperactivity Disorder; Steering Committee on Quality Improvement and Management; Wolraich M, Brown L, Brown RT, DuPaul G, Earls M, Feldman HM, Ganiats TG, Kaplanek B, Meyer B, Perrin J, Pierce K, Reiff M, Stein MT, Visser S. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics. 2011 Nov;128(5):1007-22. doi: 10.1542/peds.2011-2654. Epub 2011 Oct 16. Citation on PubMed or Free article on PubMed Central
- Sudre G, Frederick J, Sharp W, Ishii-Takahashi A, Mangalmurti A, Choudhury S, Shaw P. Mapping associations between polygenic risks for childhood neuropsychiatric disorders, symptoms of attention deficit hyperactivity disorder, cognition, and the brain. Mol Psychiatry. 2020 Oct;25(10):2482-2492. doi: 10.1038/s41380-019-0350-3. Epub 2019 Jan 30. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.