

Description
Beckwith-Wiedemann syndrome is a condition that affects many parts of the body. It is classified as an overgrowth syndrome, which means that affected infants are larger than normal (macrosomia), and some may be taller than their peers during childhood. Growth begins to slow by about age 8, and adults with this condition are not unusually tall. In some children with Beckwith-Wiedemann syndrome, specific body parts may grow abnormally large on one side of the body, leading to an asymmetric or uneven appearance. This unusual growth pattern, which is known as hemihyperplasia, usually becomes less apparent over time.
The signs and symptoms of Beckwith-Wiedemann syndrome vary among affected individuals. Some children with this condition are born with an opening in the wall of the abdomen (an omphalocele ) that allows the abdominal organs to protrude through the belly-button. Other abdominal wall defects, such as a soft out-pouching around the belly-button (an umbilical hernia
) that allows the abdominal organs to protrude through the belly-button. Other abdominal wall defects, such as a soft out-pouching around the belly-button (an umbilical hernia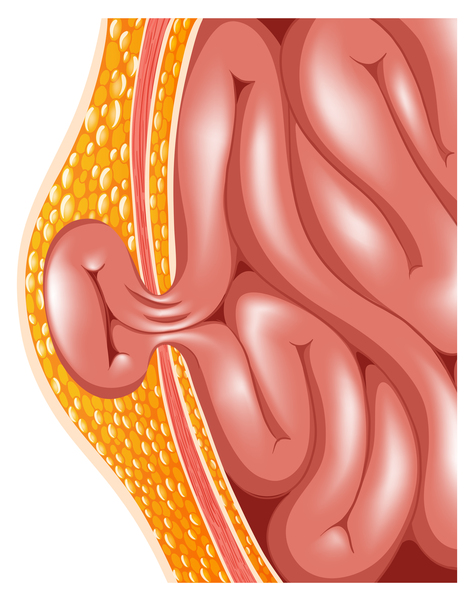 ), are also common. Some infants with Beckwith-Wiedemann syndrome have an abnormally large tongue (macroglossia
), are also common. Some infants with Beckwith-Wiedemann syndrome have an abnormally large tongue (macroglossia ), which may interfere with breathing, swallowing, and speaking. Other major features of this condition include abnormally large abdominal organs (visceromegaly), creases or pits
), which may interfere with breathing, swallowing, and speaking. Other major features of this condition include abnormally large abdominal organs (visceromegaly), creases or pits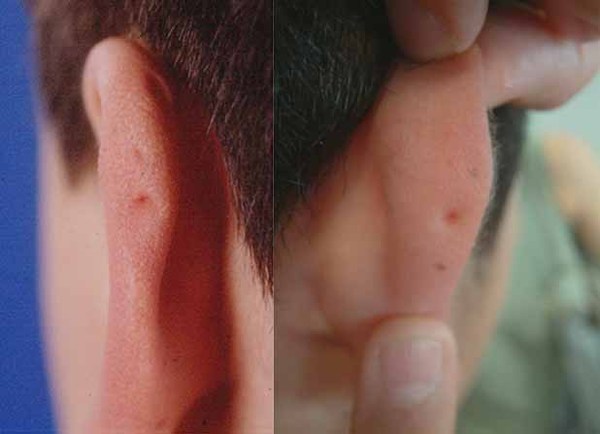 in the skin near the ears, low blood glucose (hypoglycemia) in infancy, and kidney abnormalities.
in the skin near the ears, low blood glucose (hypoglycemia) in infancy, and kidney abnormalities.
Children with Beckwith-Wiedemann syndrome are at an increased risk of developing several types of cancerous and noncancerous tumors, particularly a form of kidney cancer called Wilms tumor and a form of liver cancer called hepatoblastoma. Tumors develop in about 10 percent of people with this condition and almost always appear in childhood.
Most children and adults with Beckwith-Wiedemann syndrome do not have serious medical problems associated with the condition. Their life expectancy is usually normal.
Frequency
Beckwith-Wiedemann syndrome affects 1 in 10,500 to 13,700 newborns worldwide. The condition may actually be more common than this estimate because some people with mild symptoms are never diagnosed.
Causes
The genetic causes of Beckwith-Wiedemann syndrome are complex. The condition usually results from the abnormal regulation of genes in a particular region of chromosome 11. People normally inherit one copy of this chromosome from each parent. For most genes on chromosome 11, both copies of the gene are expressed, or "turned on," in cells. For some genes, however, only the copy inherited from a person's father (the paternally inherited copy) is expressed. For other genes, only the copy inherited from a person's mother (the maternally inherited copy) is expressed. These parent-specific differences in gene expression are caused by a phenomenon called genomic imprinting. Abnormalities involving genes on chromosome 11 that undergo genomic imprinting are responsible for most cases of Beckwith-Wiedemann syndrome.
At least half of all cases result from changes in a process called methylation. Methylation is a chemical reaction that attaches small molecules called methyl groups to certain segments of DNA. In genes that undergo genomic imprinting, methylation is one way that a gene's parent of origin is marked during the formation of egg and sperm cells. Beckwith-Wiedemann syndrome is often associated with changes in regions of DNA on chromosome 11 called imprinting centers (ICs). ICs control the methylation of several genes that are involved in normal growth, including the CDKN1C, H19, IGF2, and KCNQ1OT1 genes. Abnormal methylation disrupts the regulation of these genes, which leads to overgrowth and the other characteristic features of Beckwith-Wiedemann syndrome.
About twenty percent of cases of Beckwith-Wiedemann syndrome are caused by a genetic change known as paternal uniparental disomy (UPD). Paternal UPD causes people to have two active copies of paternally inherited genes rather than one active copy from the father and one inactive copy from the mother. People with paternal UPD are also missing genes that are active only on the maternally inherited copy of the chromosome. In Beckwith-Wiedemann syndrome, paternal UPD usually occurs early in embryonic development and affects only some of the body's cells. This phenomenon is called mosaicism
(UPD). Paternal UPD causes people to have two active copies of paternally inherited genes rather than one active copy from the father and one inactive copy from the mother. People with paternal UPD are also missing genes that are active only on the maternally inherited copy of the chromosome. In Beckwith-Wiedemann syndrome, paternal UPD usually occurs early in embryonic development and affects only some of the body's cells. This phenomenon is called mosaicism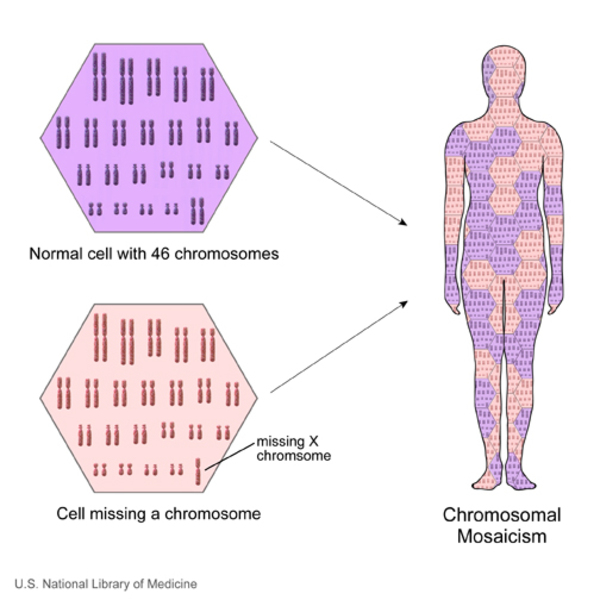 . Mosaic paternal UPD leads to an imbalance in active paternal and maternal genes on chromosome 11, which underlies the signs and symptoms of the disorder.
. Mosaic paternal UPD leads to an imbalance in active paternal and maternal genes on chromosome 11, which underlies the signs and symptoms of the disorder.
Less commonly, variants (also known as mutations) in the CDKN1C gene cause Beckwith-Wiedemann syndrome. This gene provides instructions for making a protein that helps control growth before birth. Variants in the CDKN1C gene prevent this protein from restraining growth, which leads to the abnormalities characteristic of Beckwith-Wiedemann syndrome.
Up to 6 percent of people with Beckwith-Wiedemann syndrome have a chromosomal abnormality such as a rearrangement (translocation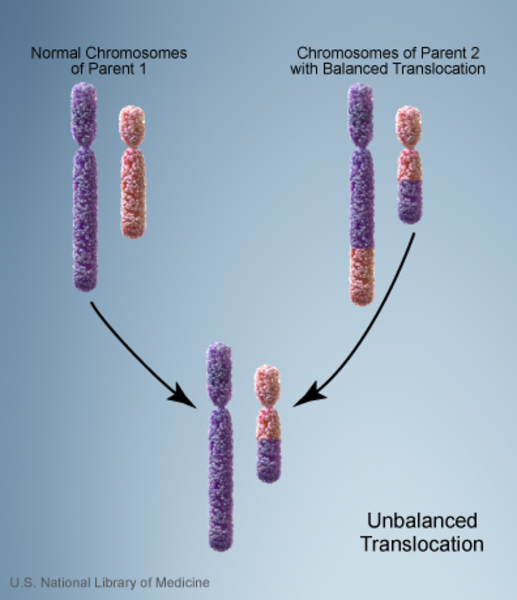 ), abnormal copying (duplication
), abnormal copying (duplication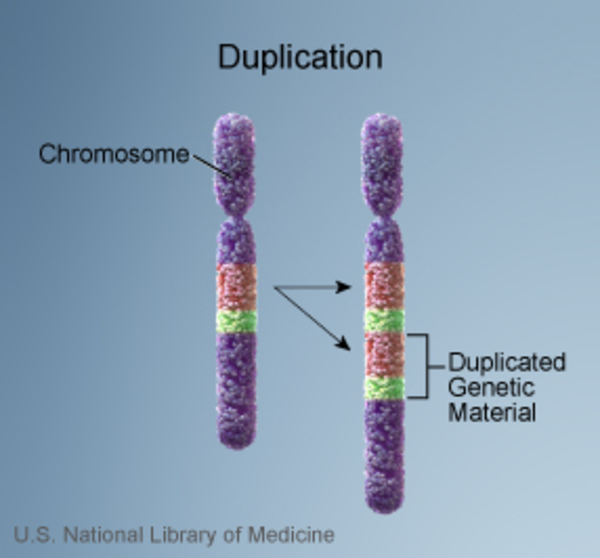 ), or loss (deletion
), or loss (deletion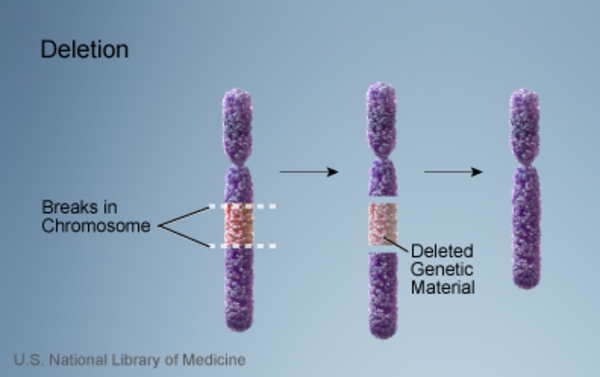 ) of genetic material from chromosome 11. Like the other genetic changes responsible for Beckwith-Wiedemann syndrome, these abnormalities disrupt the normal regulation of certain genes on this chromosome.
) of genetic material from chromosome 11. Like the other genetic changes responsible for Beckwith-Wiedemann syndrome, these abnormalities disrupt the normal regulation of certain genes on this chromosome.
Inheritance
In about 85 percent of cases of Beckwith-Wiedemann syndrome, only one person in a family has been diagnosed with the condition. However, parents of one child with Beckwith-Wiedemann syndrome may be at risk of having other children with the disorder. This risk depends on the genetic cause of the condition.
Another 10 to 15 percent of people with Beckwith-Wiedemann syndrome are part of families with more than one affected family member. In most of these families, the condition appears to have an autosomal dominant pattern of inheritance. Autosomal dominant inheritance means that one copy of an altered gene in each cell is typically sufficient to cause the disorder. A person who inherits the altered gene may not have any of the characteristic signs and symptoms of the condition, depending on which parent passed the altered copy to them. In most cases caused by CDKN1C gene variants, individuals with Beckwith-Wiedemann syndrome inherit the genetic change from their mothers.
of inheritance. Autosomal dominant inheritance means that one copy of an altered gene in each cell is typically sufficient to cause the disorder. A person who inherits the altered gene may not have any of the characteristic signs and symptoms of the condition, depending on which parent passed the altered copy to them. In most cases caused by CDKN1C gene variants, individuals with Beckwith-Wiedemann syndrome inherit the genetic change from their mothers.
Rarely, Beckwith-Wiedemann syndrome results from changes in the structure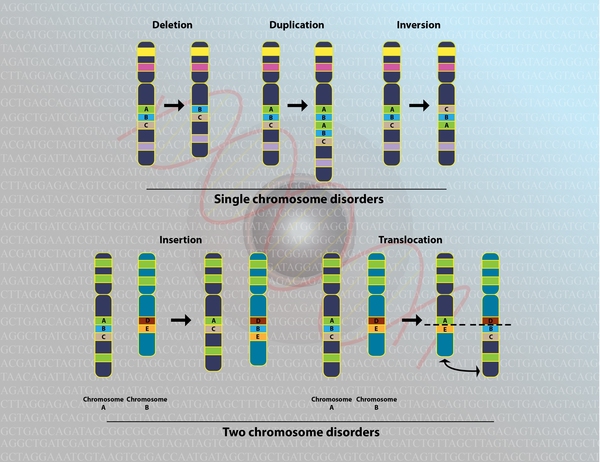 of chromosome 11. Some of these chromosomal abnormalities are inherited from a parent, while others occur as random events during the formation of reproductive cells (eggs and sperm) or in the earliest stages of development before birth.
of chromosome 11. Some of these chromosomal abnormalities are inherited from a parent, while others occur as random events during the formation of reproductive cells (eggs and sperm) or in the earliest stages of development before birth.
Other Names for This Condition
- BWS
- Wiedemann-Beckwith syndrome (WBS)
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Brioude F, Kalish JM, Mussa A, Foster AC, Bliek J, Ferrero GB, Boonen SE, Cole T, Baker R, Bertoletti M, Cocchi G, Coze C, De Pellegrin M, Hussain K, Ibrahim A, Kilby MD, Krajewska-Walasek M, Kratz CP, Ladusans EJ, Lapunzina P, Le Bouc Y, Maas SM, Macdonald F, Ounap K, Peruzzi L, Rossignol S, Russo S, Shipster C, Skorka A, Tatton-Brown K, Tenorio J, Tortora C, Gronskov K, Netchine I, Hennekam RC, Prawitt D, Tumer Z, Eggermann T, Mackay DJG, Riccio A, Maher ER. Expert consensus document: Clinical and molecular diagnosis, screening and management of Beckwith-Wiedemann syndrome: an international consensus statement. Nat Rev Endocrinol. 2018 Apr;14(4):229-249. doi: 10.1038/nrendo.2017.166. Epub 2018 Jan 29. Citation on PubMed
- Choufani S, Shuman C, Weksberg R. Beckwith-Wiedemann syndrome. Am J Med Genet C Semin Med Genet. 2010 Aug 15;154C(3):343-54. doi: 10.1002/ajmg.c.30267. Citation on PubMed
- Choufani S, Shuman C, Weksberg R. Molecular findings in Beckwith-Wiedemann syndrome. Am J Med Genet C Semin Med Genet. 2013 May;163C(2):131-40. doi: 10.1002/ajmg.c.31363. Epub 2013 Apr 16. Citation on PubMed
- Cooper WN, Curley R, Macdonald F, Maher ER. Mitotic recombination and uniparental disomy in Beckwith-Wiedemann syndrome. Genomics. 2007 May;89(5):613-7. doi: 10.1016/j.ygeno.2007.01.005. Epub 2007 Mar 6. Citation on PubMed
- Duffy KA, Cielo CM, Cohen JL, Gonzalez-Gandolfi CX, Griff JR, Hathaway ER, Kupa J, Taylor JA, Wang KH, Ganguly A, Deardorff MA, Kalish JM. Characterization of the Beckwith-Wiedemann spectrum: Diagnosis and management. Am J Med Genet C Semin Med Genet. 2019 Dec;181(4):693-708. doi: 10.1002/ajmg.c.31740. Epub 2019 Aug 30. Citation on PubMed
- Eggermann T, Algar E, Lapunzina P, Mackay D, Maher ER, Mannens M, Netchine I, Prawitt D, Riccio A, Temple IK, Weksberg R. Clinical utility gene card for: Beckwith-Wiedemann Syndrome. Eur J Hum Genet. 2014 Mar;22(3). doi: 10.1038/ejhg.2013.132. Epub 2013 Jul 3. No abstract available. Citation on PubMed or Free article on PubMed Central
- Rump P, Zeegers MP, van Essen AJ. Tumor risk in Beckwith-Wiedemann syndrome: A review and meta-analysis. Am J Med Genet A. 2005 Jul 1;136(1):95-104. doi: 10.1002/ajmg.a.30729. Citation on PubMed
- Shuman C, Kalish JM, Weksberg R. Beckwith-Wiedemann Syndrome. 2000 Mar 3 [updated 2023 Sep 21]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1394/ Citation on PubMed
- Smith AC, Choufani S, Ferreira JC, Weksberg R. Growth regulation, imprinted genes, and chromosome 11p15.5. Pediatr Res. 2007 May;61(5 Pt 2):43R-47R. doi: 10.1203/pdr.0b013e3180457660. Citation on PubMed
- Wang KH, Kupa J, Duffy KA, Kalish JM. Diagnosis and Management of Beckwith-Wiedemann Syndrome. Front Pediatr. 2020 Jan 21;7:562. doi: 10.3389/fped.2019.00562. eCollection 2019. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.