

Description
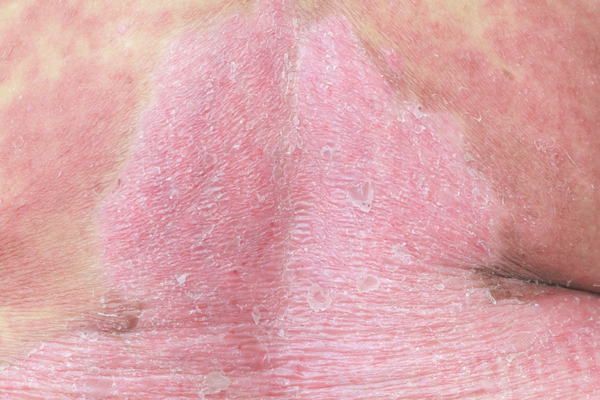
Atopic dermatitis (also known as atopic eczema) is a disorder characterized by inflammation of the skin (dermatitis). The condition usually begins in early infancy, and it often disappears before adolescence. However, in some affected individuals the condition continues into adulthood; in others, it does not begin until adulthood. Hallmarks of atopic dermatitis include dry, itchy skin and red rashes that come and go. The rashes can occur on any part of the body, although the pattern tends to be different at different ages. In affected infants, the rashes commonly occur on the face, scalp, hands, and feet. In children, the rashes are usually found in the bend of the elbows and knees and on the front of the neck. In adolescents and adults, the rashes typically occur on the wrists, ankles, and eyelids in addition to the bend of the elbows and knees. Scratching the itchy skin can lead to oozing and crusting of the rashes and thickening and hardening (lichenification) of the skin. The itchiness can be so severe as to disturb sleep and impair a person's quality of life.
The word "atopic" indicates an association with allergies. While atopic dermatitis is not always due to an allergic reaction, it is commonly associated with other allergic disorders: up to 60 percent of people with atopic dermatitis develop asthma or hay fever (allergic rhinitis) later in life, and up to 30 percent have food allergies. Atopic dermatitis is often the beginning of a series of allergic disorders, referred to as the "atopic march." Development of these disorders typically follows a pattern, beginning with atopic dermatitis, followed by food allergies, then hay fever, and finally asthma. However, not all individuals with atopic dermatitis will progress through the atopic march, and not all individuals with one allergic disease will develop others.
Individuals with atopic dermatitis have an increased risk of developing other conditions related to inflammation, such as inflammatory bowel disease, rheumatoid arthritis, and hair loss caused by a malfunctioning immune reaction (alopecia areata). They also have an increased risk of having a behavioral or psychiatric disorder, such as attention-deficit/hyperactivity disorder (ADHD) or depression.
In a particular subset of individuals with atopic dermatitis, the immune system is unable to protect the body from foreign invaders such as bacteria and fungi (which is known as immunodeficiency). These individuals are prone to recurrent infections. Most also have other allergic disorders, such as asthma, hay fever, and food allergies.
Atopic dermatitis can also be a feature of separate disorders that have a number of signs and symptoms, which can include skin abnormalities and immunodeficiency. Some such disorders are Netherton syndrome; immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome; and severe dermatitis, multiple allergies, metabolic wasting (SAM) syndrome.
Frequency
Atopic dermatitis is a common disorder that affects 10 to 20 percent of children and 5 to 10 percent of adults.
Causes
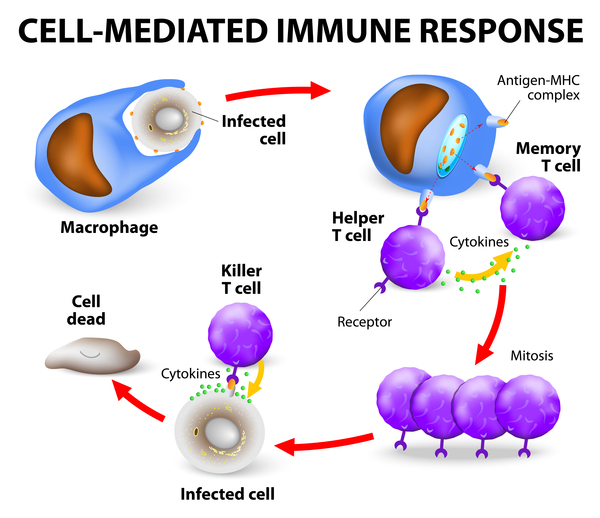
The genetics of atopic dermatitis are not completely understood. Studies suggest that several genes can be involved in development of the condition. In very rare cases, atopic dermatitis is caused by inherited mutations in a single gene. One such gene is the CARD11 gene. The protein produced from this gene turns on signaling pathways involved in the development and function of immune system cells called lymphocytes. Mutations in the CARD11 gene lead to production of an altered CARD11 protein that does not function normally. These changes impair pathway signaling, and as a result, certain lymphocytes called T cells do not develop or function properly. The number of these cells is normal, but their response to foreign invaders such as bacteria and fungi is diminished. The T cell abnormalities lead to a weakened immune system and recurrent infections, which are common in people with CARD11-associated atopic dermatitis.
It is not clear how the immune dysfunction caused by CARD11 gene mutations leads to skin rashes and allergic disorders in affected individuals. Atopic dermatitis is not initially caused by an allergic reaction, although sometimes substances that can cause allergic reactions (allergens) are thought to contribute to flare-ups of the rashes.
In contrast to rare cases caused by CARD11 gene mutations, most cases of atopic dermatitis are thought to occur due to a combination of genetic and environmental factors (such as living with a pet). Several common genetic variations may be involved, each contributing only a small amount to the risk of developing atopic dermatitis. The strongest of these associations is with the FLG gene, which is altered in 20 to 30 percent of people with atopic dermatitis compared with 8 to 10 percent of the general population without atopic dermatitis.
The FLG gene provides instructions for making a protein called profilaggrin, which is important for the structure of the outermost layer of skin. Proteins derived from profilaggrin help create a strong barrier to keep in water and keep out foreign substances, including toxins, bacteria, and allergens. These proteins also are part of the skin's "natural moisturizing factor," which helps maintain hydration of the outermost layer of skin.
Variations in the FLG gene lead to production of an abnormally short profilaggrin protein that cannot be processed to produce the other profilaggrin-related proteins. The resulting shortage can impair the barrier function of the skin. Impairment of the skin's barrier function contributes to development of allergic disorders, including atopic dermatitis. Research suggests that without a properly functioning barrier, allergens are able to get into the body through the skin, triggering a reaction. In addition, a lack of natural moisturizing factor allows excess water loss through the skin, which can lead to dry skin.
Variations in many other genes are likely associated with development of atopic dermatitis, although most of these genes have not been identified or definitively linked to the disorder. Researchers suspect these genes are involved in the skin's barrier function or in the function of the immune system. However, not everyone with a mutation in FLG or another risk-associated gene develops atopic dermatitis; exposure to certain environmental factors also contributes to the development of the disorder. Studies suggest that these exposures trigger epigenetic changes to the DNA. Epigenetic changes modify DNA without changing the DNA sequence. They can affect gene activity and regulate the production of proteins, which may influence the development of allergies in susceptible individuals.
Syndromes with atopic dermatitis as one of several features are caused by mutations in other genes.
Inheritance
Allergic disorders tend to run in families; having a parent with atopic dermatitis, asthma, or hay fever raises the chances a person will develop atopic dermatitis.
When caused by CARD11 gene mutations, atopic dermatitis has an autosomal dominant inheritance pattern, which means one copy of the altered CARD11 gene in each cell is sufficient to cause the disorder.

Similarly, when associated with FLG gene mutations, risk of the condition follows an autosomal dominant pattern; a mutation in one copy of the FLG gene is sufficient to increase the risk of the disorder. Individuals with two altered copies of the FLG gene are more likely to develop the disorder and can have more severe signs and symptoms than individuals with a single altered copy.
When atopic dermatitis is associated with other genetic factors, the inheritance pattern is unclear. While CARD11 gene mutations appear to cause the condition without other contributing factors, people with changes in the FLG gene or another atopic dermatitis-associated gene inherit an increased risk of this condition, not the condition itself. Not all people with this condition have a mutation in a risk-associated gene, and not all people with a variation in a risk-associated gene will develop the disorder.
Other Names for This Condition
- Atopic eczema
Additional Information & Resources
Genetic Testing Information
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Bieber T. Atopic dermatitis. N Engl J Med. 2008 Apr 3;358(14):1483-94. doi: 10.1056/NEJMra074081. No abstract available. Citation on PubMed
- Dadi H, Jones TA, Merico D, Sharfe N, Ovadia A, Schejter Y, Reid B, Sun M, Vong L, Atkinson A, Lavi S, Pomerantz JL, Roifman CM. Combined immunodeficiency and atopy caused by a dominant negative mutation in caspase activation and recruitment domain family member 11 (CARD11). J Allergy Clin Immunol. 2018 May;141(5):1818-1830.e2. doi: 10.1016/j.jaci.2017.06.047. Epub 2017 Aug 19. Citation on PubMed
- Irvine AD, McLean WH, Leung DY. Filaggrin mutations associated with skin and allergic diseases. N Engl J Med. 2011 Oct 6;365(14):1315-27. doi: 10.1056/NEJMra1011040. No abstract available. Citation on PubMed
- Liang Y, Chang C, Lu Q. The Genetics and Epigenetics of Atopic Dermatitis-Filaggrin and Other Polymorphisms. Clin Rev Allergy Immunol. 2016 Dec;51(3):315-328. doi: 10.1007/s12016-015-8508-5. Citation on PubMed
- Ma CA, Stinson JR, Zhang Y, Abbott JK, Weinreich MA, Hauk PJ, Reynolds PR, Lyons JJ, Nelson CG, Ruffo E, Dorjbal B, Glauzy S, Yamakawa N, Arjunaraja S, Voss K, Stoddard J, Niemela J, Zhang Y, Rosenzweig SD, McElwee JJ, DiMaggio T, Matthews HF, Jones N, Stone KD, Palma A, Oleastro M, Prieto E, Bernasconi AR, Dubra G, Danielian S, Zaiat J, Marti MA, Kim B, Cooper MA, Romberg N, Meffre E, Gelfand EW, Snow AL, Milner JD. Germline hypomorphic CARD11 mutations in severe atopic disease. Nat Genet. 2017 Aug;49(8):1192-1201. doi: 10.1038/ng.3898. Epub 2017 Jun 19. Erratum In: Nat Genet. 2017 Oct 27;49(11):1661. doi: 10.1038/ng1117-1661b. Citation on PubMed
- O'Regan GM, Irvine AD. The role of filaggrin loss-of-function mutations in atopic dermatitis. Curr Opin Allergy Clin Immunol. 2008 Oct;8(5):406-10. doi: 10.1097/ACI.0b013e32830e6fb2. Citation on PubMed
- Shaker M. New insights into the allergic march. Curr Opin Pediatr. 2014 Aug;26(4):516-20. doi: 10.1097/MOP.0000000000000120. Citation on PubMed
- Shi JH, Sun SC. TCR signaling to NF-kappaB and mTORC1: Expanding roles of the CARMA1 complex. Mol Immunol. 2015 Dec;68(2 Pt C):546-57. doi: 10.1016/j.molimm.2015.07.024. Epub 2015 Aug 8. Citation on PubMed or Free article on PubMed Central
- Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016 Mar 12;387(10023):1109-1122. doi: 10.1016/S0140-6736(15)00149-X. Epub 2015 Sep 13. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.