

Description
Transthyretin amyloidosis is a progressive condition characterized by the buildup of abnormal protein deposits called amyloids (amyloidosis) in the body's organs and tissues. These protein deposits most frequently occur in the peripheral nervous system, which is made up of nerves that connect the brain and spinal cord to muscles and sensory cells that detect sensations such as touch, pain, heat, and sound. Protein deposits in these nerves result in a loss of sensation or in muscle weakness in the extremities (peripheral neuropathy). The autonomic nervous system, which controls involuntary body functions such as blood pressure, heart rate, and digestion, may also be affected by amyloidosis. In some cases, the brain and spinal cord (central nervous system) are affected. Other areas of amyloidosis include the heart, kidneys, eyes, and gastrointestinal tract. The age at which symptoms begin to develop varies widely among individuals with this condition, typically ranging from age 20 to 70.
There are two major forms of transthyretin amyloidosis, which are distinguished by their symptoms and the body systems they affect.
The neuropathic form of transthyretin amyloidosis primarily affects the peripheral and autonomic nervous systems, resulting in peripheral neuropathy and difficulty controlling bodily functions. Impairments to bodily functions can include sexual impotence, diarrhea, constipation, problems with urination, and a sharp drop in blood pressure upon standing (orthostatic hypotension). Some people experience heart and kidney problems as well. Various eye problems may occur, such as cloudiness of the clear gel that fills the eyeball (vitreous opacity), dry eyes, increased pressure in the eyes (glaucoma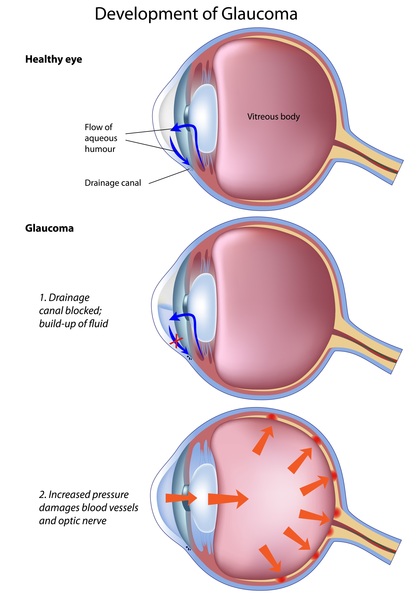 ), or pupils with an irregular or "scalloped" appearance. Some people with this form of transthyretin amyloidosis develop carpal tunnel syndrome, which is characterized by numbness, tingling, and weakness in the hands and fingers.
), or pupils with an irregular or "scalloped" appearance. Some people with this form of transthyretin amyloidosis develop carpal tunnel syndrome, which is characterized by numbness, tingling, and weakness in the hands and fingers.
The cardiac form of transthyretin amyloidosis affects the heart. People with cardiac amyloidosis may have an abnormal heartbeat (arrhythmia), an enlarged heart (cardiomegaly), or orthostatic hypertension. These abnormalities can lead to progressive heart failure and death. Occasionally, people with the cardiac form of transthyretin amyloidosis have mild peripheral neuropathy.
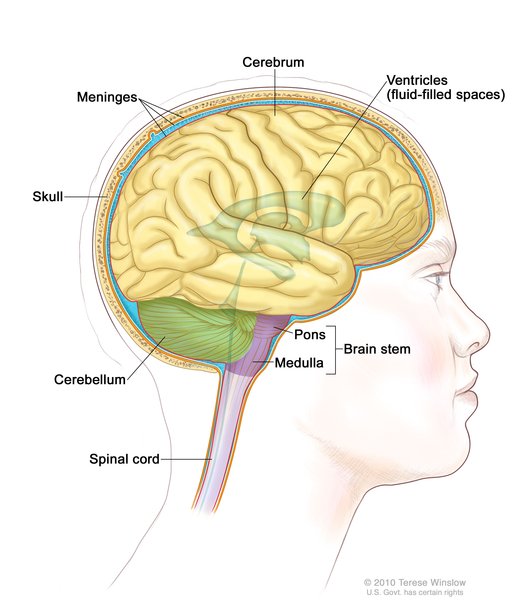
A less common form of transthyretin amyloidosis, called the leptomeningeal form, primarily affects the central nervous system. In people with this form, amyloidosis occurs in the leptomeninges, which are two thin layers of tissue that cover the brain and spinal cord. A buildup of proteins in this tissue can cause stroke and bleeding in the brain, an accumulation of fluid in the brain (hydrocephalus), difficulty coordinating movements (ataxia), muscle stiffness and weakness (spastic paralysis), seizures, and loss of intellectual function (dementia). Eye problems similar to those seen in the neuropathic form of transthyretin amyloidosis may also occur; people with leptomeningeal transthyretin amyloidosis who have these eye problems are said to have the oculoleptomeningeal form.
Frequency
The exact incidence of transthyretin amyloidosis is unknown. In northern Portugal, the incidence of this condition is thought to be one in 538 people. Transthyretin amyloidosis is less common among Americans of European descent, where it is estimated to affect one in 100,000 people. The cardiac form of transthyretin amyloidosis is more common among people with African ancestry. It is estimated that this form affects between 3 percent and 3.9 percent of African Americans and approximately 5 percent of people in some areas of West Africa.
Causes
Variants (also called mutations) in the TTR gene cause transthyretin amyloidosis. The TTR gene provides instructions for making a protein called transthyretin. Transthyretin transports vitamin A (retinol) and a hormone called thyroxine throughout the body. To transport retinol and thyroxine, four transthyretin proteins must attach (bind) to each other to form a four-protein unit (tetramer).
The TTR gene variants that cause transthyretin amyloidosis alter the structure of transthyretin, impairing its ability to form tetramers. As a result, the tetramers break down into individual transthyretin proteins, which attach to each other in strands called fibrils. The fibrils clump together and form amyloid deposits in certain tissues, leading to the signs and symptoms of transthyretin amyloidosis.
Inheritance
This condition is inherited in an autosomal dominant pattern , which means one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases, an affected person inherits the variant from one affected parent. Rarely, the condition results from a new (de novo) variant
, which means one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases, an affected person inherits the variant from one affected parent. Rarely, the condition results from a new (de novo) variant in the gene that occur during the formation of reproductive cells (eggs or sperm) in an affected individual's parent or in early embryonic development. These affected individuals have no history of the disorder in their family. Not all people who have a TTR gene variant will develop transthyretin amyloidosis.
in the gene that occur during the formation of reproductive cells (eggs or sperm) in an affected individual's parent or in early embryonic development. These affected individuals have no history of the disorder in their family. Not all people who have a TTR gene variant will develop transthyretin amyloidosis.
Other Names for This Condition
- ATTR
- hATTR
- Portuguese polyneuritic amyloidosis
- Portuguese type familial amyloid neuropathy
- Swiss type amyloid polyneuropathy
- Type I familial amyloid polyneuropathy
- Type II familial amyloid polyneuropathy
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Ando Y, Nakamura M, Araki S. Transthyretin-related familial amyloidotic polyneuropathy. Arch Neurol. 2005 Jul;62(7):1057-62. doi: 10.1001/archneur.62.7.1057. Citation on PubMed
- Benson MD, Kincaid JC. The molecular biology and clinical features of amyloid neuropathy. Muscle Nerve. 2007 Oct;36(4):411-23. doi: 10.1002/mus.20821. Citation on PubMed
- Hou X, Aguilar MI, Small DH. Transthyretin and familial amyloidotic polyneuropathy. Recent progress in understanding the molecular mechanism of neurodegeneration. FEBS J. 2007 Apr;274(7):1637-50. doi: 10.1111/j.1742-4658.2007.05712.x. Citation on PubMed
- Joao Saraiva M, Mendes Sousa M, Cardoso I, Fernandes R. Familial amyloidotic polyneuropathy: protein aggregation in the peripheral nervous system. J Mol Neurosci. 2004;23(1-2):35-40. doi: 10.1385/jmn:23:1-2:035. Citation on PubMed
- Plante-Bordeneuve V, Said G. Transthyretin related familial amyloid polyneuropathy. Curr Opin Neurol. 2000 Oct;13(5):569-73. doi: 10.1097/00019052-200010000-00011. Citation on PubMed
- Saraiva MJ. Hereditary transthyretin amyloidosis: molecular basis and therapeutical strategies. Expert Rev Mol Med. 2002 May 14;4(12):1-11. doi: 10.1017/S1462399402004647. Citation on PubMed
- Sekijima Y, Nakamura K. Hereditary Transthyretin Amyloidosis. 2001 Nov 5 [updated 2024 May 30]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1194/ Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.