

Description
Arginine vasopressin deficiency (previously called neurohypophyseal diabetes insipidus) is a disorder of water balance. The body normally balances fluid intake by releasing fluid in urine. However, people with arginine vasopressin deficiency produce an excessive amount of urine (polyuria), which depletes the amount of water in the body. This water loss also leads to excessive thirst (polydipsia).
People with arginine vasopressin deficiency can quickly become dehydrated if they do not drink enough water. Dehydration can cause dizziness and fatigue. Prolonged dehydration can lead to confusion, low blood pressure, seizures, and coma. People with this condition often develop high levels of sodium in the blood (hypernatremia) due to dehydration. Repeated cycles of dehydration can cause long-term health problems, particularly in children.
Arginine vasopressin deficiency can be either acquired or familial. The acquired form occurs when the brain is damaged due to head injuries, brain tumors, or other events, and this form can occur at any time during life. The familial form is caused by genetic changes; its signs and symptoms usually become apparent in childhood and worsen over time.
Researchers have recommended using the condition name arginine vasopressin deficiency because the previous name, neurohypophyseal diabetes insipidus, was often confused with a much more common disorder called diabetes mellitus.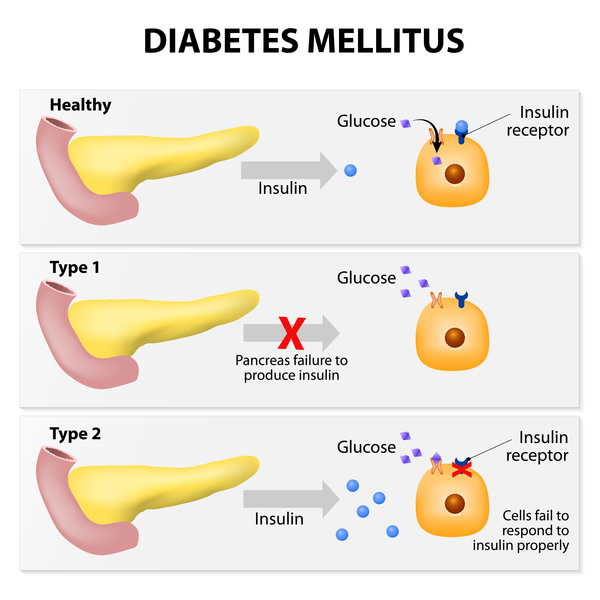 Arginine vasopressin deficiency and diabetes mellitus are separate disorders with different features, causes, and treatment.
Arginine vasopressin deficiency and diabetes mellitus are separate disorders with different features, causes, and treatment.
Frequency
Arginine vasopressin deficiency occurs in approximately 1 in 25,000 individuals. The acquired form is much more common than the familial form.
Causes
The familial form of arginine vasopressin deficiency is caused by variants (also called mutations) in the AVP gene. This gene provides instructions for making a hormone called arginine vasopressin (AVP), which is sometimes also called antidiuretic hormone (ADH). This hormone, which is produced and stored in the brain, helps control the body's water balance.
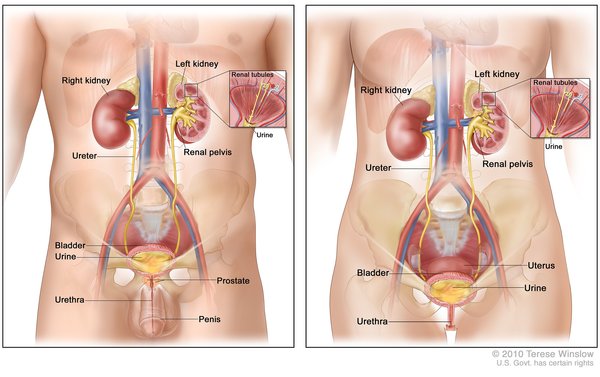
AVP works with the kidneys to manage the balance between fluid reabsorption and fluid release. Normally, when a person's fluid intake is low or when a lot of fluid is lost (for example, through sweating), the brain releases more AVP into the bloodstream. High levels of this hormone direct the kidneys to reabsorb more water and to make less urine. When fluid intake is adequate, the brain releases less AVP.
Variants in the AVP gene result in the production of an AVP hormone that does not get released from brain cells. Without this hormone, the kidneys do not reabsorb water as they should, and the body makes excessive amounts of urine. These problems with water balance are characteristic of arginine vasopressin deficiency.
The acquired form of arginine vasopressin deficiency occurs when the areas of the brain that produce or store AVP are damaged by head injuries, brain tumors, brain surgery, certain diseases and infections, or bleeding in the brain. A loss of AVP disrupts the body's water balance, leading to excessive urine production and the other features of the disorder.
In 30 to 50 percent of all cases of arginine vasopressin deficiency, the cause of the disorder is unknown. Studies suggest that some of these cases may be caused by a malfunctioning immune system that attacks the body's own tissues and organs.
Inheritance
Familial arginine vasopressin deficiency is almost always inherited in an autosomal dominant pattern , which means that one copy of the altered AVP gene in each cell is sufficient to cause the disorder.
, which means that one copy of the altered AVP gene in each cell is sufficient to cause the disorder.
In a few affected families, familial arginine vasopressin deficiency has had an autosomal recessive pattern of inheritance. Autosomal recessive inheritance means that both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
of inheritance. Autosomal recessive inheritance means that both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- Central diabetes insipidus
- Diabetes insipidus secondary to vasopressin deficiency
- Diabetes insipidus, central
- Diabetes insipidus, neurogenic
- Diabetes insipidus, neurohypophyseal
- Diabetes insipidus, pituitary
- Neurohypophyseal diabetes insipidus
- Pituitary diabetes insipidus
- Vasopressin defective diabetes insipidus
- Vasopressin deficiency
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Atila C, Loughrey PB, Garrahy A, Winzeler B, Refardt J, Gildroy P, Hamza M, Pal A, Verbalis JG, Thompson CJ, Hemkens LG, Hunter SJ, Sherlock M, Levy MJ, Karavitaki N, Newell-Price J, Wass JAH, Christ-Crain M. Central diabetes insipidus from a patient's perspective: management, psychological co-morbidities, and renaming of the condition: results from an international web-based survey. Lancet Diabetes Endocrinol. 2022 Oct;10(10):700-709. doi: 10.1016/S2213-8587(22)00219-4. Epub 2022 Aug 22. Citation on PubMed
- Baldeweg SE, Ball S, Brooke A, Gleeson HK, Levy MJ, Prentice M, Wass J; Society for Endocrinology Clinical Committee. SOCIETY FOR ENDOCRINOLOGY CLINICAL GUIDANCE: Inpatient management of cranial diabetes insipidus. Endocr Connect. 2018 Jul;7(7):G8-G11. doi: 10.1530/EC-18-0154. Citation on PubMed
- Christensen JH, Rittig S. Familial neurohypophyseal diabetes insipidus--an update. Semin Nephrol. 2006 May;26(3):209-23. doi: 10.1016/j.semnephrol.2006.03.003. Citation on PubMed
- Fujiwara TM, Bichet DG. Molecular biology of hereditary diabetes insipidus. J Am Soc Nephrol. 2005 Oct;16(10):2836-46. doi: 10.1681/ASN.2005040371. Epub 2005 Aug 10. Citation on PubMed
- Ghirardello S, Garre ML, Rossi A, Maghnie M. The diagnosis of children with central diabetes insipidus. J Pediatr Endocrinol Metab. 2007 Mar;20(3):359-75. doi: 10.1515/jpem.2007.20.3.359. Citation on PubMed
- Ghirardello S, Malattia C, Scagnelli P, Maghnie M. Current perspective on the pathogenesis of central diabetes insipidus. J Pediatr Endocrinol Metab. 2005 Jul;18(7):631-45. doi: 10.1515/jpem.2005.18.7.631. Citation on PubMed
- Maghnie M, Cosi G, Genovese E, Manca-Bitti ML, Cohen A, Zecca S, Tinelli C, Gallucci M, Bernasconi S, Boscherini B, Severi F, Arico M. Central diabetes insipidus in children and young adults. N Engl J Med. 2000 Oct 5;343(14):998-1007. doi: 10.1056/NEJM200010053431403. Citation on PubMed
- Pivonello R, De Bellis A, Faggiano A, Di Salle F, Petretta M, Di Somma C, Perrino S, Altucci P, Bizzarro A, Bellastella A, Lombardi G, Colao A. Central diabetes insipidus and autoimmunity: relationship between the occurrence of antibodies to arginine vasopressin-secreting cells and clinical, immunological, and radiological features in a large cohort of patients with central diabetes insipidus of known and unknown etiology. J Clin Endocrinol Metab. 2003 Apr;88(4):1629-36. doi: 10.1210/jc.2002-020791. Citation on PubMed
- Refardt J, Atila C, Christ-Crain M. New insights on diagnosis and treatment of AVP deficiency. Rev Endocr Metab Disord. 2024 Jun;25(3):639-649. doi: 10.1007/s11154-023-09862-w. Epub 2023 Dec 13. Citation on PubMed
- Teare H, Argente J, Dattani M, Leger J, Maghnie M, Sherlock M, Ali GC, Francombe J, Marjanovic S. Challenges and improvement needs in the care of patients with central diabetes insipidus. Orphanet J Rare Dis. 2022 Feb 16;17(1):58. doi: 10.1186/s13023-022-02191-2. Citation on PubMed
- Tomkins M, Lawless S, Martin-Grace J, Sherlock M, Thompson CJ. Diagnosis and Management of Central Diabetes Insipidus in Adults. J Clin Endocrinol Metab. 2022 Sep 28;107(10):2701-2715. doi: 10.1210/clinem/dgac381. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.