

Description
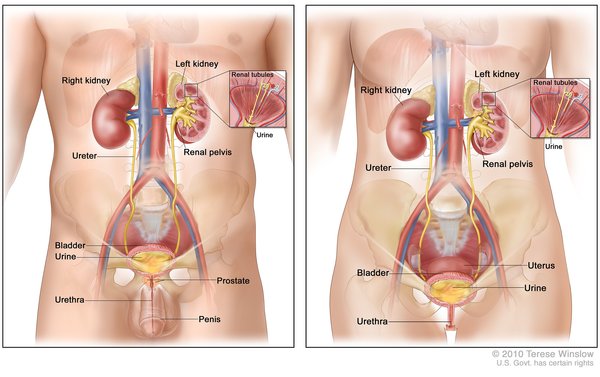
Kidney stones (also called renal stones or urinary stones) are small, hard deposits that form in one or both kidneys; the stones are made up of minerals or other compounds found in urine. Kidney stones vary in size, shape, and color. To be cleared from the body (or "passed"), the stones need to travel through ducts that carry urine from the kidneys to the bladder (ureters) and be excreted. Depending on their size, kidney stones generally take days to weeks to pass out of the body.
Kidney stones can cause abdominal or back pain (known as renal colic). Renal colic usually begins sporadically but then becomes constant and can lead to nausea and vomiting. The site of pain can change as the stone moves through the urinary tract. Some small stones pass through the kidney and urinary tract with little discomfort, while larger ones can block the flow of urine and impair kidney function. Kidney stones can also result in blood in the urine (hematuria) or kidney or urinary tract infections. Unusually large stones or stones that are difficult to pass can be medically removed.
Although there are many types of kidney stones, four main types are classified by the material they are made of. Up to 75 percent of all kidney stones are composed primarily of calcium. Stones can also be made up of uric acid (a normal waste product), cystine (a protein building block), or struvite (a phosphate mineral). Stones form when there is more of the compound in the urine than can be dissolved. This imbalance can occur when there is an increased amount of the material in the urine, a reduced amount of liquid urine, or a combination of both.
People are most likely to develop kidney stones between ages 40 and 60, though the stones can appear at any age. Research shows that 35 to 50 percent of people who have one kidney stone will develop additional stones, usually within 10 years of the first stone.
Frequency
In the United States, 9 percent of women and 19 percent of men develop kidney stones in their lifetime. Caucasians are more likely to develop kidney stones than African Americans.
Causes
Genetic changes can increase the risk of developing kidney stones, often acting in combination with a variety of environmental and lifestyle factors. Most genes involved in the condition are important for transmitting chemical signals from outside cells to inside cells or transporting materials in and out of cells. These processes help regulate the levels of various materials within cells, including the minerals and compounds that make up kidney stones. Changes in these genes can alter the levels of these materials in cells, leading to an imbalance of minerals and compounds in urine. As a result, the likelihood of stone formation increases.
A key factor that contributes to the development of kidney stones is too little water in the body (dehydration). When a person is dehydrated, they excrete less water in their urine, so the urine becomes concentrated with minerals and compounds that can cluster to form stones. Eating certain foods, such as animal proteins or foods high in sodium, can increase the likelihood of developing stones. A diet deficient in calcium can increase levels of other substances that cause stone development in individuals who have a history of kidney stones. Additionally, people who take certain medications, such as diuretics, which help remove water and salt from the body through urine, or calcium antacids, which treat indigestion by neutralizing stomach acids, are more likely to develop kidney stones.
In most cases, kidney stones occur without any other health issues. However, some people develop kidney stones as part of another condition. About half of people who develop calcium stones have high levels of calcium in the urine (hypercalciuria). Hypercalciuria often runs in families. Some other health conditions that increase the risk of kidney stones include obesity, type 2 diabetes, inflammatory bowel disease (abnormal inflammation of the intestinal walls), gout (abnormal inflammation in the joints caused by high levels of uric acid in the blood), hyperparathyroidism (overactivity of the parathyroid glands), renal tubular acidosis (kidney dysfunction that leads to too much acid in the blood), and recurrent urinary tract infections.
Inheritance
The inheritance pattern of kidney stones is unclear. Overall, the risk of developing this condition is greater for individuals who have a close relative (such as a parent or sibling) with the condition as compared to the general public.
Other Names for This Condition
- Calculus of kidney
- Calculus, kidney
- Calculus, renal
- Kidney calculi
- Kidney stone
- Nephrolith
- Nephrolithiasis
- Renal calculi
- Renal calculus
- Renal lithiasis
- Renal stones
- Urinary stones
- Urolithiasis
Additional Information & Resources
Genetic Testing Information
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, Pace KT, Pais VM Jr, Pearle MS, Preminger GM, Razvi H, Shah O, Matlaga BR. Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART I. J Urol. 2016 Oct;196(4):1153-60. doi: 10.1016/j.juro.2016.05.090. Epub 2016 May 27. Citation on PubMed
- Assimos D, Krambeck A, Miller NL, Monga M, Murad MH, Nelson CP, Pace KT, Pais VM Jr, Pearle MS, Preminger GM, Razvi H, Shah O, Matlaga BR. Surgical Management of Stones: American Urological Association/Endourological Society Guideline, PART II. J Urol. 2016 Oct;196(4):1161-9. doi: 10.1016/j.juro.2016.05.091. Epub 2016 May 27. Citation on PubMed
- Coe FL, Worcester EM, Evan AP. Idiopathic hypercalciuria and formation of calcium renal stones. Nat Rev Nephrol. 2016 Sep;12(9):519-33. doi: 10.1038/nrneph.2016.101. Epub 2016 Jul 25. Citation on PubMed or Free article on PubMed Central
- Dawson PA, Sim P, Mudge DW, Cowley D. Human SLC26A1 gene variants: a pilot study. ScientificWorldJournal. 2013 Oct 22;2013:541710. doi: 10.1155/2013/541710. eCollection 2013. Citation on PubMed or Free article on PubMed Central
- Gee HY, Jun I, Braun DA, Lawson JA, Halbritter J, Shril S, Nelson CP, Tan W, Stein D, Wassner AJ, Ferguson MA, Gucev Z, Sayer JA, Milosevic D, Baum M, Tasic V, Lee MG, Hildebrandt F. Mutations in SLC26A1 Cause Nephrolithiasis. Am J Hum Genet. 2016 Jun 2;98(6):1228-1234. doi: 10.1016/j.ajhg.2016.03.026. Epub 2016 May 19. Citation on PubMed or Free article on PubMed Central
- Maalouf NM. Nephrolithiasis. 2026 Feb 6. In: Feingold KR, Adler RA, Ahmed SF, Anawalt B, Blackman MR, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hamilton E, Hofland J, Jan de Beur S, Kalra S, Kaltsas G, Kapoor N, Kim M, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrere B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Sperling MA, Stratakis CA, Trence DL, Wilson DP, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from http://www.ncbi.nlm.nih.gov/books/NBK279069/ Citation on PubMed
- Pearle MS, Goldfarb DS, Assimos DG, Curhan G, Denu-Ciocca CJ, Matlaga BR, Monga M, Penniston KL, Preminger GM, Turk TM, White JR; American Urological Assocation. Medical management of kidney stones: AUA guideline. J Urol. 2014 Aug;192(2):316-24. doi: 10.1016/j.juro.2014.05.006. Epub 2014 May 20. Citation on PubMed
- Qaseem A, Dallas P, Forciea MA, Starkey M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Dietary and pharmacologic management to prevent recurrent nephrolithiasis in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2014 Nov 4;161(9):659-67. doi: 10.7326/M13-2908. Citation on PubMed
- Taguchi K, Yasui T, Milliner DS, Hoppe B, Chi T. Genetic Risk Factors for Idiopathic Urolithiasis: A Systematic Review of the Literature and Causal Network Analysis. Eur Urol Focus. 2017 Feb;3(1):72-81. doi: 10.1016/j.euf.2017.04.010. Epub 2017 May 19. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.