

Description
X-linked acrogigantism (X-LAG) is a condition that causes abnormally fast growth beginning early in life. Babies with this condition are a normal size at birth but begin to grow rapidly in infancy or early childhood, and affected children are taller than their peers.
This rapid growth is caused by an abnormality of the pituitary gland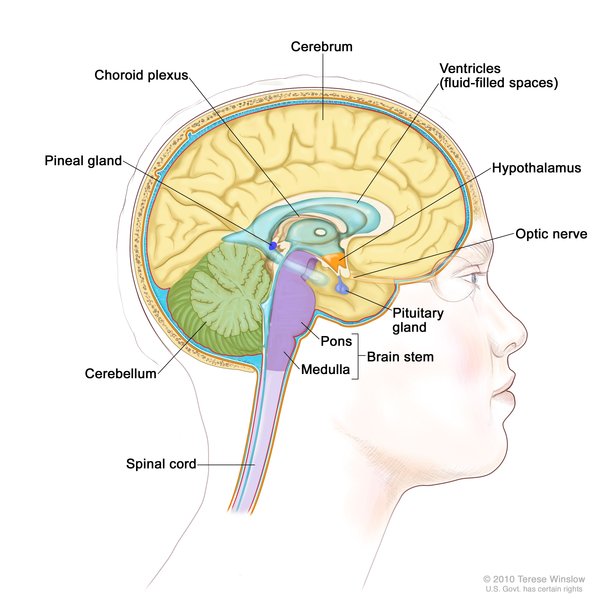 . The pituitary gland, which is found at the base of the brain, produces hormones that control many important body functions, including growth. Individuals with X-LAG may have the condition as a result of enlargement (hyperplasia) of the gland or development of a noncancerous tumor in the gland (called a pituitary neuroendocrine tumor or PitNET). Rarely, an affected individual has both pituitary hyperplasia and a pituitary neuroendocrine tumor. The abnormal gland releases excess amounts of growth hormone, a hormone that normally helps direct growth of the body's bones and tissues. The abnormal gland can also release excess amounts of another hormone called prolactin, which helps control the function of the internal reproductive organs (gonads).
. The pituitary gland, which is found at the base of the brain, produces hormones that control many important body functions, including growth. Individuals with X-LAG may have the condition as a result of enlargement (hyperplasia) of the gland or development of a noncancerous tumor in the gland (called a pituitary neuroendocrine tumor or PitNET). Rarely, an affected individual has both pituitary hyperplasia and a pituitary neuroendocrine tumor. The abnormal gland releases excess amounts of growth hormone, a hormone that normally helps direct growth of the body's bones and tissues. The abnormal gland can also release excess amounts of another hormone called prolactin, which helps control the function of the internal reproductive organs (gonads).
Some people with X-LAG have additional signs and symptoms such as facial features that are described as coarse; disproportionately large hands or feet (acral enlargement); an increased appetite; and a skin condition called acanthosis nigricans, in which the skin in body folds and creases becomes thick, dark, and velvety.
Frequency
X-LAG is thought to be a very rare condition, although the prevalence is not known. It occurs more frequently in females than in males. X-LAG accounts for one in ten cases of abnormally fast growth in children that is caused by pituitary gland abnormalities (pituitary gigantism).
Causes
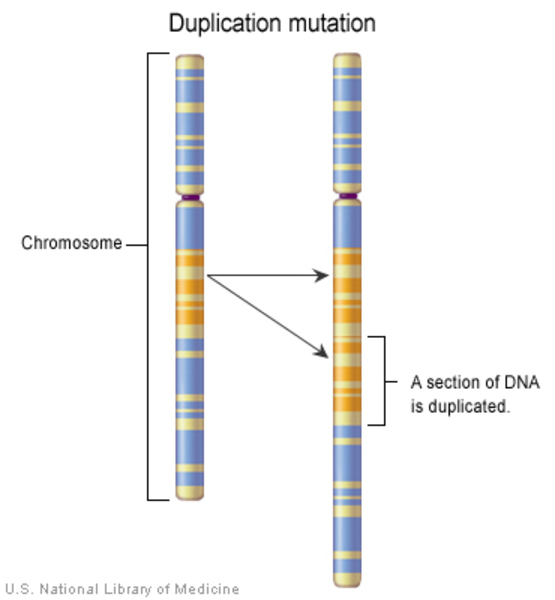
X-LAG is caused by a genetic change in which a small amount of genetic material on the X chromosome is abnormally copied (duplicated). The duplication, often referred to as an Xq26.3 microduplication, occurs on the long (q) arm of the chromosome at a location designated q26.3. It can include several genes, but only duplication of the GPR101 gene is necessary to cause X-LAG.
The GPR101 gene provides instructions for making a protein whose function is unknown. Studies suggest that the GPR101 protein is involved in the growth of cells in the pituitary gland or in the release of growth hormone from the gland.
Duplication of the GPR101 gene leads to an excess of GPR101 protein. It is unclear how extra GPR101 protein results in the development of a pituitary adenoma or hyperplasia or in the release of excess growth hormone or GHRH.
Inheritance
X-LAG follows an X-linked dominant inheritance pattern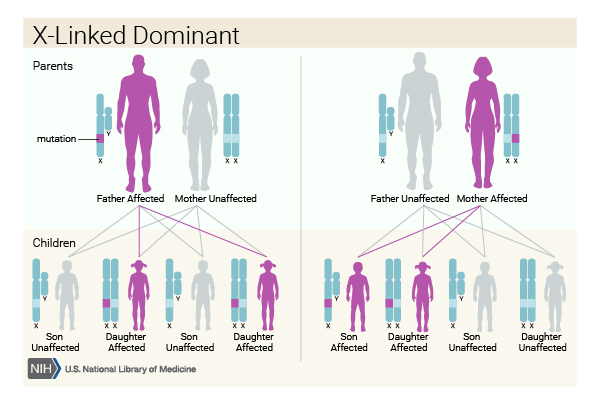 . The gene associated with this condition is located on the X chromosome, which is one of the two sex chromosomes
. The gene associated with this condition is located on the X chromosome, which is one of the two sex chromosomes . In females (who have two X chromosomes), a duplication of one of the two copies of the GPR101 gene in each cell is sufficient to cause the disorder. In males (who have only one X chromosome), a duplication of the only copy of the gene in each cell causes the disorder. A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons.
. In females (who have two X chromosomes), a duplication of one of the two copies of the GPR101 gene in each cell is sufficient to cause the disorder. In males (who have only one X chromosome), a duplication of the only copy of the gene in each cell causes the disorder. A characteristic of X-linked inheritance is that fathers cannot pass X-linked traits to their sons.
In females, the condition results from new (de novo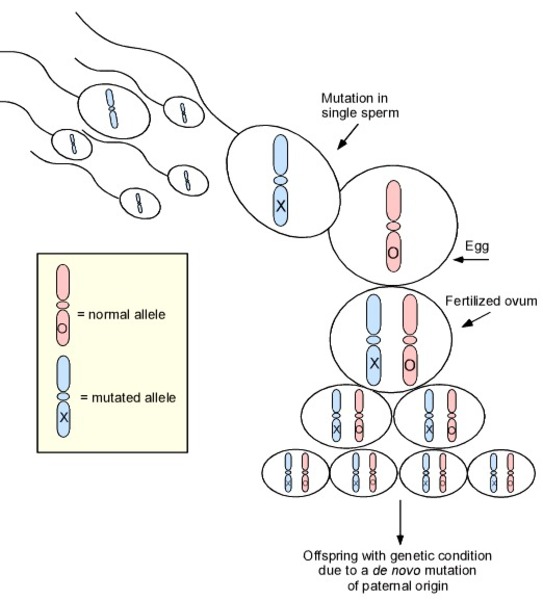 ) duplications involving the GPR101 gene that occur during the formation of a parent's reproductive cells (eggs or sperm). The duplication is found in all of the cells in the affected person's body.
) duplications involving the GPR101 gene that occur during the formation of a parent's reproductive cells (eggs or sperm). The duplication is found in all of the cells in the affected person's body.
In males, the condition often results from somatic mosaicism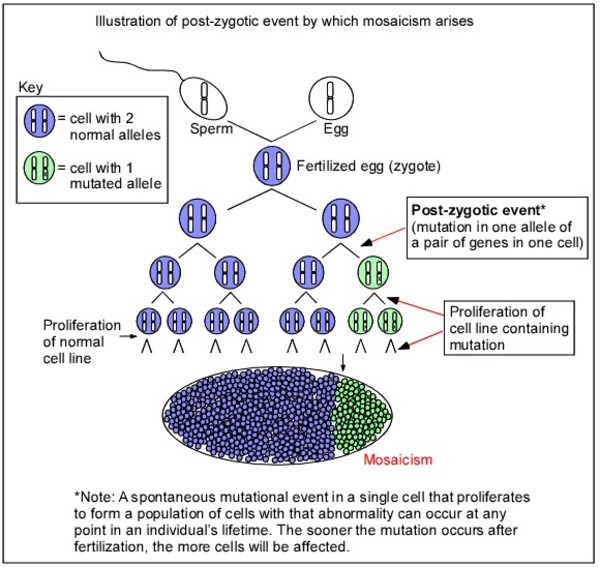 , in which some of an affected person's cells have the duplication and others do not. The genetic changes, which are called somatic variants, arise randomly in one cell during embryonic development. As cells continue to divide, only cells arising from the first abnormal cell will have the variant. Other affected males inherit the duplication from their affected mother, and it is found in all the body's cells.
, in which some of an affected person's cells have the duplication and others do not. The genetic changes, which are called somatic variants, arise randomly in one cell during embryonic development. As cells continue to divide, only cells arising from the first abnormal cell will have the variant. Other affected males inherit the duplication from their affected mother, and it is found in all the body's cells.
Other Names for This Condition
- Chromosome Xq26 microduplication syndrome
- Chromosome Xq26.3 duplication syndrome
- X-LAG
- X-linked acrogigantism syndrome
- XLAG
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Beckers A, Lodish MB, Trivellin G, Rostomyan L, Lee M, Faucz FR, Yuan B, Choong CS, Caberg JH, Verrua E, Naves LA, Cheetham TD, Young J, Lysy PA, Petrossians P, Cotterill A, Shah NS, Metzger D, Castermans E, Ambrosio MR, Villa C, Strebkova N, Mazerkina N, Gaillard S, Barra GB, Casulari LA, Neggers SJ, Salvatori R, Jaffrain-Rea ML, Zacharin M, Santamaria BL, Zacharieva S, Lim EM, Mantovani G, Zatelli MC, Collins MT, Bonneville JF, Quezado M, Chittiboina P, Oldfield EH, Bours V, Liu P, W de Herder W, Pellegata N, Lupski JR, Daly AF, Stratakis CA. X-linked acrogigantism syndrome: clinical profile and therapeutic responses. Endocr Relat Cancer. 2015 Jun;22(3):353-67. doi: 10.1530/ERC-15-0038. Epub 2015 Feb 24. Citation on PubMed or Free article on PubMed Central
- Daly AF, Lysy PA, Desfilles C, Rostomyan L, Mohamed A, Caberg JH, Raverot V, Castermans E, Marbaix E, Maiter D, Brunelle C, Trivellin G, Stratakis CA, Bours V, Raftopoulos C, Beauloye V, Barlier A, Beckers A. GHRH excess and blockade in X-LAG syndrome. Endocr Relat Cancer. 2016 Mar;23(3):161-70. doi: 10.1530/ERC-15-0478. Epub 2015 Dec 15. Citation on PubMed
- Daly AF, Yuan B, Fina F, Caberg JH, Trivellin G, Rostomyan L, de Herder WW, Naves LA, Metzger D, Cuny T, Rabl W, Shah N, Jaffrain-Rea ML, Zatelli MC, Faucz FR, Castermans E, Nanni-Metellus I, Lodish M, Muhammad A, Palmeira L, Potorac I, Mantovani G, Neggers SJ, Klein M, Barlier A, Liu P, Ouafik L, Bours V, Lupski JR, Stratakis CA, Beckers A. Somatic mosaicism underlies X-linked acrogigantism syndrome in sporadic male subjects. Endocr Relat Cancer. 2016 Apr;23(4):221-33. doi: 10.1530/ERC-16-0082. Epub 2016 Mar 2. Citation on PubMed or Free article on PubMed Central
- Iacovazzo D, Caswell R, Bunce B, Jose S, Yuan B, Hernandez-Ramirez LC, Kapur S, Caimari F, Evanson J, Ferrau F, Dang MN, Gabrovska P, Larkin SJ, Ansorge O, Rodd C, Vance ML, Ramirez-Renteria C, Mercado M, Goldstone AP, Buchfelder M, Burren CP, Gurlek A, Dutta P, Choong CS, Cheetham T, Trivellin G, Stratakis CA, Lopes MB, Grossman AB, Trouillas J, Lupski JR, Ellard S, Sampson JR, Roncaroli F, Korbonits M. Germline or somatic GPR101 duplication leads to X-linked acrogigantism: a clinico-pathological and genetic study. Acta Neuropathol Commun. 2016 Jun 1;4(1):56. doi: 10.1186/s40478-016-0328-1. Citation on PubMed or Free article on PubMed Central
- Rodd C, Millette M, Iacovazzo D, Stiles CE, Barry S, Evanson J, Albrecht S, Caswell R, Bunce B, Jose S, Trouillas J, Roncaroli F, Sampson J, Ellard S, Korbonits M. Somatic GPR101 Duplication Causing X-Linked Acrogigantism (XLAG)-Diagnosis and Management. J Clin Endocrinol Metab. 2016 May;101(5):1927-30. doi: 10.1210/jc.2015-4366. Epub 2016 Mar 16. Citation on PubMed or Free article on PubMed Central
- Rostomyan L, Daly AF, Petrossians P, Nachev E, Lila AR, Lecoq AL, Lecumberri B, Trivellin G, Salvatori R, Moraitis AG, Holdaway I, Kranenburg-van Klaveren DJ, Chiara Zatelli M, Palacios N, Nozieres C, Zacharin M, Ebeling T, Ojaniemi M, Rozhinskaya L, Verrua E, Jaffrain-Rea ML, Filipponi S, Gusakova D, Pronin V, Bertherat J, Belaya Z, Ilovayskaya I, Sahnoun-Fathallah M, Sievers C, Stalla GK, Castermans E, Caberg JH, Sorkina E, Auriemma RS, Mittal S, Kareva M, Lysy PA, Emy P, De Menis E, Choong CS, Mantovani G, Bours V, De Herder W, Brue T, Barlier A, Neggers SJ, Zacharieva S, Chanson P, Shah NS, Stratakis CA, Naves LA, Beckers A. Clinical and genetic characterization of pituitary gigantism: an international collaborative study in 208 patients. Endocr Relat Cancer. 2015 Oct;22(5):745-57. doi: 10.1530/ERC-15-0320. Epub 2015 Jul 17. Citation on PubMed
- Trivellin G, Bjelobaba I, Daly AF, Larco DO, Palmeira L, Faucz FR, Thiry A, Leal LF, Rostomyan L, Quezado M, Schernthaner-Reiter MH, Janjic MM, Villa C, Wu TJ, Stojilkovic SS, Beckers A, Feldman B, Stratakis CA. Characterization of GPR101 transcript structure and expression patterns. J Mol Endocrinol. 2016 Aug;57(2):97-111. doi: 10.1530/JME-16-0045. Epub 2016 Jun 9. Citation on PubMed or Free article on PubMed Central
- Trivellin G, Daly AF, Faucz FR, Yuan B, Rostomyan L, Larco DO, Schernthaner-Reiter MH, Szarek E, Leal LF, Caberg JH, Castermans E, Villa C, Dimopoulos A, Chittiboina P, Xekouki P, Shah N, Metzger D, Lysy PA, Ferrante E, Strebkova N, Mazerkina N, Zatelli MC, Lodish M, Horvath A, de Alexandre RB, Manning AD, Levy I, Keil MF, Sierra Mde L, Palmeira L, Coppieters W, Georges M, Naves LA, Jamar M, Bours V, Wu TJ, Choong CS, Bertherat J, Chanson P, Kamenicky P, Farrell WE, Barlier A, Quezado M, Bjelobaba I, Stojilkovic SS, Wess J, Costanzi S, Liu P, Lupski JR, Beckers A, Stratakis CA. Gigantism and acromegaly due to Xq26 microduplications and GPR101 mutation. N Engl J Med. 2014 Dec 18;371(25):2363-74. doi: 10.1056/NEJMoa1408028. Epub 2014 Dec 3. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.