

Description
Schimke immuno-osseous dysplasia is a condition characterized by short stature, kidney disease, and a weakened immune system. People with this condition have flattened spinal bones (vertebrae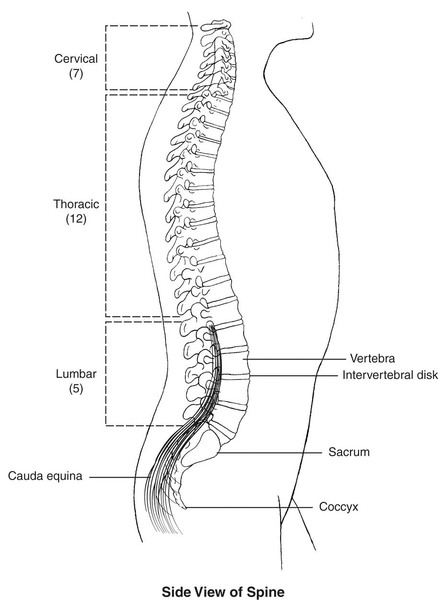 ) that shorten their neck and trunk. The adult height for people with this condition is typically between 3 and 5 feet. Additional skeletal problems in people with Schimke immuno-osseous dysplasia include abnormalities of the hip joints and the end of the leg bones where they meet the hip joint. These skeletal problems can cause the hip joints to break down (degenerate) over time, leading to joint pain and a limited range of movement. This combination of skeletal problems and spinal abnormalities is called spondyloepiphyseal dysplasia as it affects the bones of the spine (spondylo-) and the ends of long bones (epiphyses
) that shorten their neck and trunk. The adult height for people with this condition is typically between 3 and 5 feet. Additional skeletal problems in people with Schimke immuno-osseous dysplasia include abnormalities of the hip joints and the end of the leg bones where they meet the hip joint. These skeletal problems can cause the hip joints to break down (degenerate) over time, leading to joint pain and a limited range of movement. This combination of skeletal problems and spinal abnormalities is called spondyloepiphyseal dysplasia as it affects the bones of the spine (spondylo-) and the ends of long bones (epiphyses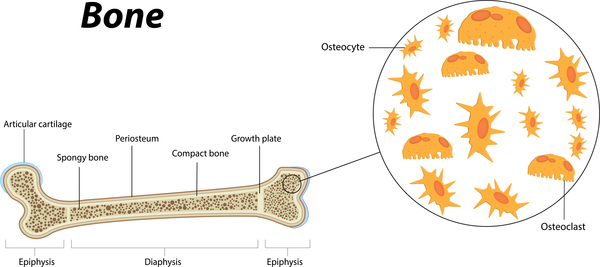 ) in the legs. It affects most people with Schimke immuno-osseous dysplasia.
) in the legs. It affects most people with Schimke immuno-osseous dysplasia.
People with Schimke immuno-osseous dysplasia often have kidney (renal) disease that may lead to life-threatening renal failure and end-stage renal disease (ESRD).
Individuals with Schimke immuno-osseous dysplasia also have a shortage of immune system cells called T cells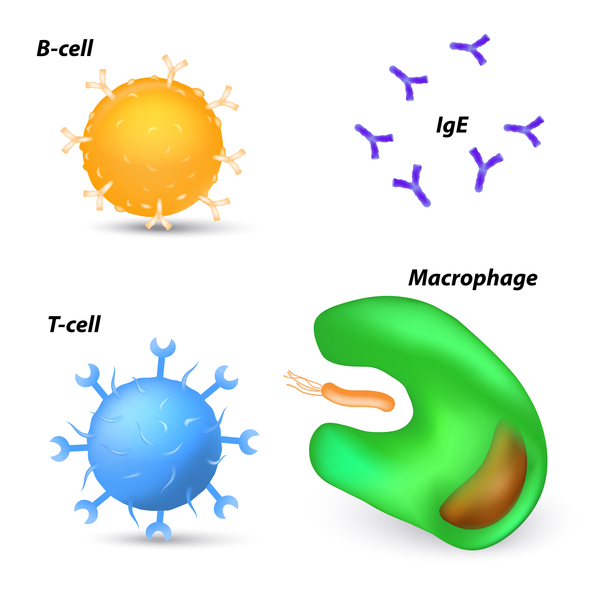 . T cells identify foreign substances and defend the body against infection. This shortage of T cells causes people with Schimke immuno-osseous dysplasia to have recurrent infections.
. T cells identify foreign substances and defend the body against infection. This shortage of T cells causes people with Schimke immuno-osseous dysplasia to have recurrent infections.
Other features frequently seen in people with Schimke immuno-osseous dysplasia include an exaggerated curvature of the lower back (lordosis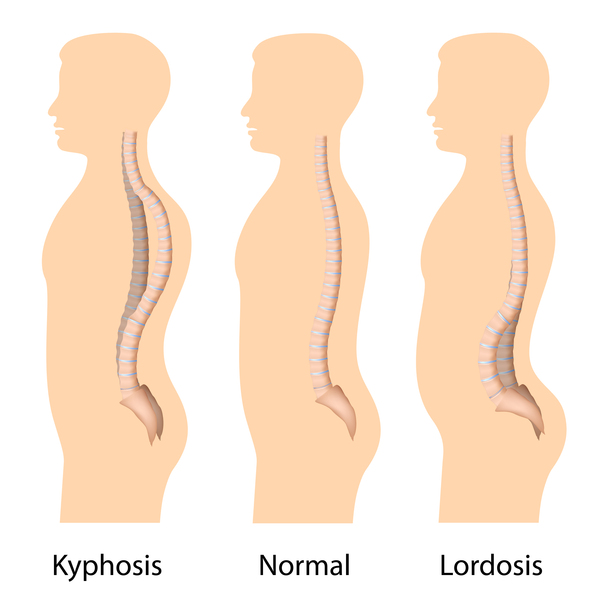 ); darkened patches of skin (hyperpigmentation), typically on the chest and back; abnormalities of the teeth; and a broad nasal bridge with a rounded tip of the nose.
); darkened patches of skin (hyperpigmentation), typically on the chest and back; abnormalities of the teeth; and a broad nasal bridge with a rounded tip of the nose.
Less common signs and symptoms of Schimke immuno-osseous dysplasia include an accumulation of fatty deposits in the lining of the arteries (atherosclerosis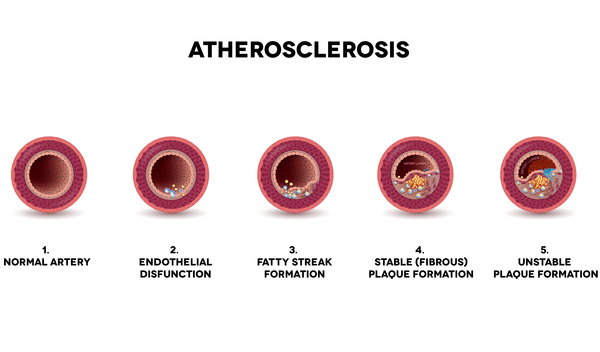 ), reduced blood flow to the brain (ischemic stroke
), reduced blood flow to the brain (ischemic stroke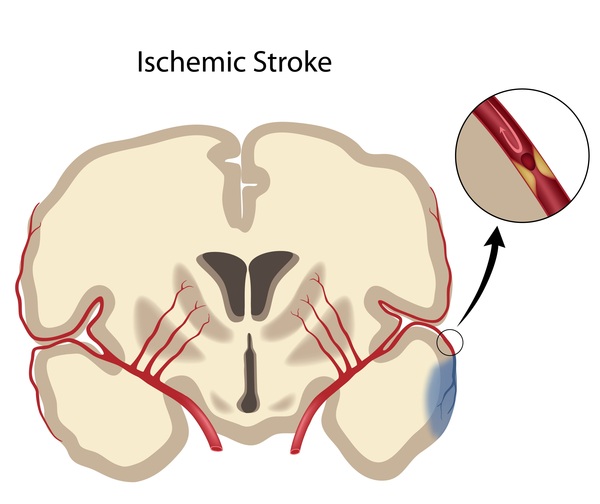 ), migraine-like headaches, an underactive thyroid gland
), migraine-like headaches, an underactive thyroid gland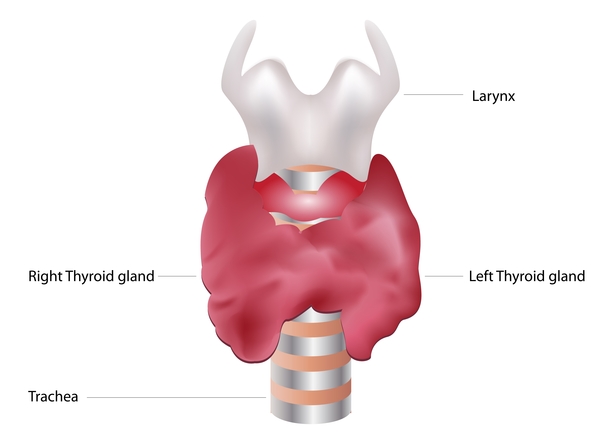 (hypothyroidism), a decrease in the number of blood cells (anemia), a lack of sperm (azoospermia), and irregular menstruation.
(hypothyroidism), a decrease in the number of blood cells (anemia), a lack of sperm (azoospermia), and irregular menstruation.
In severe cases, individuals with Schimke immuno-osseous dysplasia do not survive past childhood. In mild cases, people with Schimke immuno-osseous dysplasia can survive into adulthood.
Frequency
Schimke immuno-osseous dysplasia is a very rare condition. The prevalence is estimated to be 1 in 1 million to 3 million people.
Causes
Variants (also called mutations) in the SMARCAL1 gene can cause Schimke immuno-osseous dysplasia. The SMARCAL1 gene provides instructions for producing a protein that interacts with DNA. The SMARCAL1 protein helps when the process of making new copies of DNA, called DNA replication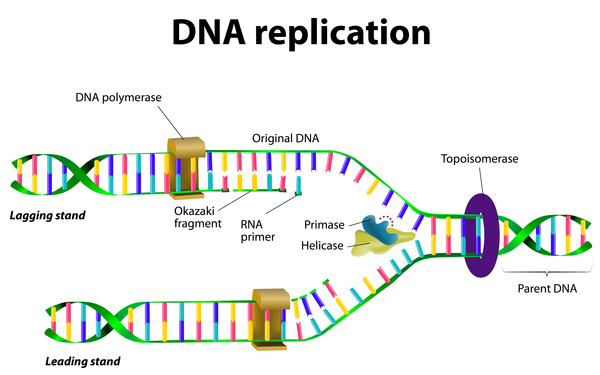 , is blocked by DNA damage. When DNA replication stalls, the SMARCAL1 proteins repair DNA damage by reattaching the two strands of DNA's double helix and allowing replication to proceed. Research on the function of similar proteins suggests that SMARCAL1 can influence the activity (expression) of other genes.
, is blocked by DNA damage. When DNA replication stalls, the SMARCAL1 proteins repair DNA damage by reattaching the two strands of DNA's double helix and allowing replication to proceed. Research on the function of similar proteins suggests that SMARCAL1 can influence the activity (expression) of other genes.
The altered or missing SMARCAL1 protein cannot repair DNA damage, which stalls DNA replication. While the exact mechanisms are unclear, this disruption in DNA replication and the buildup of DNA damage appears to lead to the characteristic features of Schimke immuno-osseous dysplasia. Affected individuals who have no functional SMARCAL1 proteins tend to have a more severe form of Schimke immuno-osseous dysplasia than those who have malfunctioning proteins.
Some people with Schimke immuno-osseous dysplasia do not have identified variants in the SMARCAL1 gene. In these cases, the cause of the disease is unknown.
Inheritance
This condition is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- Immunoosseous dysplasia, Schimke type
- Schimke immunoosseous dysplasia
- SIOD
- SMARCAL1-related immuno-osseous dysplasia (Schimke type)
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Bansal R, Hussain S, Chanana UB, Bisht D, Goel I, Muthuswami R. SMARCAL1, the annealing helicase and the transcriptional co-regulator. IUBMB Life. 2020 Oct;72(10):2080-2096. doi: 10.1002/iub.2354. Epub 2020 Aug 5. Citation on PubMed
- Beleford DT, Diab M, Qubty WF, Malloy MJ, Long RK, Shieh JT. Schimke immunoosseous dysplasia and management considerations for vascular risks. Am J Med Genet A. 2019 Jul;179(7):1246-1252. doi: 10.1002/ajmg.a.61148. Epub 2019 Apr 30. Citation on PubMed
- Boerkoel CF, Takashima H, John J, Yan J, Stankiewicz P, Rosenbarker L, Andre JL, Bogdanovic R, Burguet A, Cockfield S, Cordeiro I, Frund S, Illies F, Joseph M, Kaitila I, Lama G, Loirat C, McLeod DR, Milford DV, Petty EM, Rodrigo F, Saraiva JM, Schmidt B, Smith GC, Spranger J, Stein A, Thiele H, Tizard J, Weksberg R, Lupski JR, Stockton DW. Mutant chromatin remodeling protein SMARCAL1 causes Schimke immuno-osseous dysplasia. Nat Genet. 2002 Feb;30(2):215-20. doi: 10.1038/ng821. Epub 2002 Jan 22. Citation on PubMed
- Clewing JM, Fryssira H, Goodman D, Smithson SF, Sloan EA, Lou S, Huang Y, Choi K, Lucke T, Alpay H, Andre JL, Asakura Y, Biebuyck-Gouge N, Bogdanovic R, Bonneau D, Cancrini C, Cochat P, Cockfield S, Collard L, Cordeiro I, Cormier-Daire V, Cransberg K, Cutka K, Deschenes G, Ehrich JH, Frund S, Georgaki H, Guillen-Navarro E, Hinkelmann B, Kanariou M, Kasap B, Kilic SS, Lama G, Lamfers P, Loirat C, Majore S, Milford D, Morin D, Ozdemir N, Pontz BF, Proesmans W, Psoni S, Reichenbach H, Reif S, Rusu C, Saraiva JM, Sakallioglu O, Schmidt B, Shoemaker L, Sigaudy S, Smith G, Sotsiou F, Stajic N, Stein A, Stray-Pedersen A, Taha D, Taque S, Tizard J, Tsimaratos M, Wong NA, Boerkoel CF. Schimke immunoosseous dysplasia: suggestions of genetic diversity. Hum Mutat. 2007 Mar;28(3):273-83. doi: 10.1002/humu.20432. Citation on PubMed
- Deguchi K, Clewing JM, Elizondo LI, Hirano R, Huang C, Choi K, Sloan EA, Lucke T, Marwedel KM, Powell RD Jr, Santa Cruz K, Willaime-Morawek S, Inoue K, Lou S, Northrop JL, Kanemura Y, van der Kooy D, Okano H, Armstrong DL, Boerkoel CF. Neurologic phenotype of Schimke immuno-osseous dysplasia and neurodevelopmental expression of SMARCAL1. J Neuropathol Exp Neurol. 2008 Jun;67(6):565-77. doi: 10.1097/NEN.0b013e3181772777. Citation on PubMed
- Elizondo LI, Cho KS, Zhang W, Yan J, Huang C, Huang Y, Choi K, Sloan EA, Deguchi K, Lou S, Baradaran-Heravi A, Takashima H, Lucke T, Quiocho FA, Boerkoel CF. Schimke immuno-osseous dysplasia: SMARCAL1 loss-of-function and phenotypic correlation. J Med Genet. 2009 Jan;46(1):49-59. doi: 10.1136/jmg.2008.060095. Epub 2008 Sep 19. Citation on PubMed
- Lippner E, Lucke T, Salgado C, Boerkoel C, Lewis DB. Schimke Immunoosseous Dysplasia. 2002 Oct 1 [updated 2023 Mar 30]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1376/ Citation on PubMed
- Lou S, Lamfers P, McGuire N, Boerkoel CF. Longevity in Schimke immuno-osseous dysplasia. J Med Genet. 2002 Dec;39(12):922-5. doi: 10.1136/jmg.39.12.922. No abstract available. Citation on PubMed or Free article on PubMed Central
- Lucke T, Clewing JM, Boerkoel CF, Hartmann H, Das AM, Knauth M, Becker H, Donnerstag F. Cerebellar atrophy in Schimke-immuno-osseous dysplasia. Am J Med Genet A. 2007 Sep 1;143A(17):2040-5. doi: 10.1002/ajmg.a.31878. Citation on PubMed
- Merli P, Guzzo I, Locatelli F. Sequential Stem Cell-Kidney Transplantation in Schimke Immuno-osseous Dysplasia. N Engl J Med. 2022 Sep 1;387(9):859. doi: 10.1056/NEJMc2209527. No abstract available. Citation on PubMed
- Zieg J, Bezdicka M, Nemcikova M, Balascakova M, Sukova M, Sterbova K, Vondrak K, Dusek J, Krepelova A. Schimke immunoosseous dysplasia: an ultra-rare disease. a 20-year case series from the tertiary hospital in the Czech Republic. Ital J Pediatr. 2023 Jan 19;49(1):11. doi: 10.1186/s13052-023-01413-y. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.