

Description
SATB2-associated syndrome is a condition that affects several body systems. It is characterized by intellectual disability, severe speech problems, dental abnormalities, abnormalities of the head and face (craniofacial anomalies), and behavioral problems. Some of the common features can be described using the acronym SATB2 (which is the name of the gene involved in the condition): severe speech anomalies, abnormalities of the palate, teeth anomalies, behavioral issues with or without bone or brain anomalies, and onset before age 2.
Individuals with SATB2-associated syndrome typically have mild to severe intellectual disability, and their ability to speak is delayed or absent. Development of motor skills, such as rolling over, sitting, and walking, can also be delayed. Many affected individuals have behavioral problems, including hyperactivity and aggression. Some exhibit autistic behaviors, such as repetitive movements. A happy or overly friendly personality is also common among individuals with SATB2-associated syndrome. Less common neurological problems include feeding difficulties and weak muscle tone (hypotonia) in infancy. About half of affected individuals have abnormalities in the structure of the brain.
The most common craniofacial anomalies in people with SATB2-associated syndrome are a high arch or an opening in the roof of the mouth (high-arched or cleft palate
or cleft palate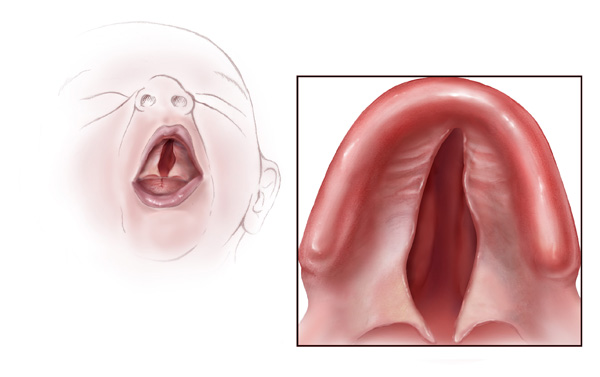 ), a small lower jaw (micrognathia), and dental abnormalities, which can include abnormally sized or shaped teeth, extra (supernumerary) teeth, or missing teeth (oligodontia). Some people with SATB2-associated syndrome have other unusual facial features, such as a prominent forehead, low-set ears, or a large area between the nose and mouth (a long philtrum
), a small lower jaw (micrognathia), and dental abnormalities, which can include abnormally sized or shaped teeth, extra (supernumerary) teeth, or missing teeth (oligodontia). Some people with SATB2-associated syndrome have other unusual facial features, such as a prominent forehead, low-set ears, or a large area between the nose and mouth (a long philtrum ). People with this disorder may also have a shortage of minerals, such as calcium, in bones (decreased bone mineral density), which makes the bones brittle and prone to fracture.
). People with this disorder may also have a shortage of minerals, such as calcium, in bones (decreased bone mineral density), which makes the bones brittle and prone to fracture.
Less-commonly affected are the heart, genitals and urinary tract (genitourinary tract), skin, and hair.
Frequency
SATB2-associated syndrome is a rare condition. Its prevalence is unknown.
Causes
SATB2-associated syndrome is caused by genetic changes that affect the SATB2 gene. These include changes within the SATB2 gene itself and deletions of large pieces of DNA from chromosome 2 that remove the SATB2 gene and other nearby genes. The SATB2 gene provides instructions for making a protein that is involved in the development of the brain and structures in the head and face. The SATB2 protein directs development by controlling the activity of multiple genes in a coordinated fashion.
Researchers suspect that genetic changes affecting the SATB2 gene reduce the amount of functional SATB2 protein. Reduction of SATB2 function likely impairs normal development of the brain and craniofacial structures, leading to intellectual disability, delayed speech, craniofacial anomalies, and other features of SATB2-associated syndrome.
The signs and symptoms of SATB2-associated syndrome are usually similar, regardless of the type of alteration that causes it. However, uncommon features of the condition, such as problems with the heart, genitourinary tract, skin, or hair, tend to occur in individuals with large deletions. Researchers suspect these features are related to the loss of other genes near SATB2.
Inheritance
SATB2-associated syndrome is not typically inherited. It results from new (de novo) changes in the gene that occur during the formation of reproductive cells (eggs or sperm) or in early embryonic development. Affected individuals have no history of the disorder in their family.
Other Names for This Condition
- 2q32 deletion syndrome
- 2q33.1 microdeletion syndrome
- Chromosome 2q32-q33 deletion syndrome
- Glass syndrome
- SAS
Additional Information & Resources
Genetic Testing Information
Patient Support and Advocacy Resources
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Bengani H, Handley M, Alvi M, Ibitoye R, Lees M, Lynch SA, Lam W, Fannemel M, Nordgren A, Malmgren H, Kvarnung M, Mehta S, McKee S, Whiteford M, Stewart F, Connell F, Clayton-Smith J, Mansour S, Mohammed S, Fryer A, Morton J; UK10K Consortium; Grozeva D, Asam T, Moore D, Sifrim A, McRae J, Hurles ME, Firth HV, Raymond FL, Kini U, Nellaker C, Ddd Study, FitzPatrick DR. Clinical and molecular consequences of disease-associated de novo mutations in SATB2. Genet Med. 2017 Aug;19(8):900-908. doi: 10.1038/gim.2016.211. Epub 2017 Feb 2. Citation on PubMed
- Britanova O, Akopov S, Lukyanov S, Gruss P, Tarabykin V. Novel transcription factor Satb2 interacts with matrix attachment region DNA elements in a tissue-specific manner and demonstrates cell-type-dependent expression in the developing mouse CNS. Eur J Neurosci. 2005 Feb;21(3):658-68. doi: 10.1111/j.1460-9568.2005.03897.x. Citation on PubMed
- Britanova O, de Juan Romero C, Cheung A, Kwan KY, Schwark M, Gyorgy A, Vogel T, Akopov S, Mitkovski M, Agoston D, Sestan N, Molnar Z, Tarabykin V. Satb2 is a postmitotic determinant for upper-layer neuron specification in the neocortex. Neuron. 2008 Feb 7;57(3):378-92. doi: 10.1016/j.neuron.2007.12.028. Citation on PubMed
- Britanova O, Depew MJ, Schwark M, Thomas BL, Miletich I, Sharpe P, Tarabykin V. Satb2 haploinsufficiency phenocopies 2q32-q33 deletions, whereas loss suggests a fundamental role in the coordination of jaw development. Am J Hum Genet. 2006 Oct;79(4):668-78. doi: 10.1086/508214. Epub 2006 Aug 30. Citation on PubMed or Free article on PubMed Central
- Dobreva G, Chahrour M, Dautzenberg M, Chirivella L, Kanzler B, Farinas I, Karsenty G, Grosschedl R. SATB2 is a multifunctional determinant of craniofacial patterning and osteoblast differentiation. Cell. 2006 Jun 2;125(5):971-86. doi: 10.1016/j.cell.2006.05.012. Citation on PubMed
- Mouille M, Rio M, Breton S, Piketty ML, Afenjar A, Amiel J, Capri Y, Goldenberg A, Francannet C, Michot C, Mignot C, Perrin L, Quelin C, Van Gils J, Barcia G, Pingault V, Maruani G, Koumakis E, Cormier-Daire V. SATB2-associated syndrome: characterization of skeletal features and of bone fragility in a prospective cohort of 19 patients. Orphanet J Rare Dis. 2022 Mar 3;17(1):100. doi: 10.1186/s13023-022-02229-5. Citation on PubMed
- Zarate YA, Fish JL. SATB2-associated syndrome: Mechanisms, phenotype, and practical recommendations. Am J Med Genet A. 2017 Feb;173(2):327-337. doi: 10.1002/ajmg.a.38022. Epub 2016 Oct 24. Citation on PubMed
- Zarate YA, Kalsner L, Basinger A, Jones JR, Li C, Szybowska M, Xu ZL, Vergano S, Caffrey AR, Gonzalez CV, Dubbs H, Zackai E, Millan F, Telegrafi A, Baskin B, Person R, Fish JL, Everman DB. Genotype and phenotype in 12 additional individuals with SATB2-associated syndrome. Clin Genet. 2017 Oct;92(4):423-429. doi: 10.1111/cge.12982. Epub 2017 Mar 7. Citation on PubMed
- Zarate YA, Steinraths M, Matthews A, Smith WE, Sun A, Wilson LC, Brain C, Allgove J, Jacobs B, Fish JL, Powell CM, Wasserman WW, van Karnebeek CD, Wakeling EL, Ma NS. Bone health and SATB2-associated syndrome. Clin Genet. 2018 Mar;93(3):588-594. doi: 10.1111/cge.13121. Epub 2017 Dec 27. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.