

Description
Metabolic dysfunction-associated steatotic liver disease (MASLD) is a condition that is characterized by a buildup of fat in the liver, which can lead to liver damage. The liver is part of the digestive system, and it helps break down food, store energy, and remove waste products. If more than 5 percent of the liver contains fat, the liver is considered to be fatty (steatotic).
MASLD is most common among middle-aged or older people, although younger people, including children, may also be affected. People with MASLD have liver steatosis along with at least one of the following features: higher body weight, type 2 diabetes, or one of several metabolic abnormalities. The abnormalities that are included in the diagnosis of MASLD are pre-diabetes (insulin resistance), high levels of fats (lipids) such as cholesterol and triglycerides in the blood, or high blood pressure (hypertension). MASLD is estimated to occur in up to 75 percent of adults with obesity or high levels of lipids in the blood and in up to 65 percent of adults with type 2 diabetes.
and triglycerides in the blood, or high blood pressure (hypertension). MASLD is estimated to occur in up to 75 percent of adults with obesity or high levels of lipids in the blood and in up to 65 percent of adults with type 2 diabetes.
In people with MASLD, the fat deposits in the liver can cause increased levels of liver enzymes that can be detected during routine blood tests. Some affected individuals have abdominal pain or fatigue. During a physical examination, the liver may be found to be slightly enlarged. In people with MASLD, the liver problems are not caused by alcohol use disorder.
MASLD is slow to worsen, or it may not worsen at all. In many affected individuals, the buildup of fat in the liver can be reduced by adopting healthy habits. However, up to 30 percent of people with MASLD develop inflammation of the liver (metabolic dysfunction-associated steatohepatitis, also known as MASH), which can damage the liver. In people with long-term liver damage, normal liver tissue may be replaced with scar tissue (fibrosis), resulting in permanent liver disease (cirrhosis) and, eventually, liver failure. People with MASLD, MASH, and cirrhosis have a higher risk of developing liver cancer (hepatocellular cancer). People with MASLD are also at increased risk of developing additional health problems such as heart (cardiovascular) disease.
Frequency
MASLD occurs in about 25 percent adults and 7 to 14 percent of children worldwide. It is the most common chronic liver disorder in Western countries, including the United States, and its prevalence is increasing along with the rising prevalence of obesity. It is estimated that MASLD will affect over half of individuals by 2040.
Causes
The specific causes of MASLD are unclear, although this condition is likely a result of both environmental factors and changes in several genes. Genetic changes that increase the risk of disease are called pathogenic variants.
When the amount of fat in a person's diet exceeds the amount the body can use, some of the fat is stored in the liver. Researchers suggest that a diet that is high in cholesterol, the refined sugars used in processed foods, and certain other nutrients may increase the likelihood of developing MASLD.
It is unclear what causes MASH and cirrhosis to develop in some people with MASLD. Researchers are studying several possible mechanisms. These include inflammation caused by an immune system reaction to the buildup of fat in the liver, toxic inflammatory chemicals (cytokines) released by the liver cells or fat cells, the self-destruction (apoptosis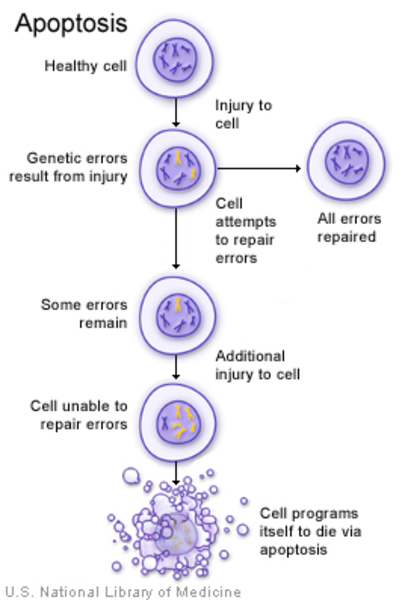 ) of liver cells, and the effect of unstable molecules called free radicals (oxidative stress). The different populations of microorganisms in the intestines (gut microbiota) may also play a role in the development of MASLD and its progression to MASH.
) of liver cells, and the effect of unstable molecules called free radicals (oxidative stress). The different populations of microorganisms in the intestines (gut microbiota) may also play a role in the development of MASLD and its progression to MASH.
Studies have identified many genetic changes that may be associated with the development of MASLD and MASH. Among these is a particular variant in the PNPLA3 gene. This gene provides instructions for making an enzyme that is found in fat and liver cells. The PNPLA3 enzyme likely helps process and store fats from the diet. The PNPLA3 gene variant that is associated with MASLD is thought to cause cells to produce an altered version of the enzyme that increases fat retention and decreases breakdown of fats in the liver. Genetic variants seem to only play a small role in the development of MASLD. Ongoing research will show how additional genetic changes contribute to the development of MASLD and its complications.
Inheritance
An increased risk of developing MASLD can be passed down through generations in families, but the inheritance pattern is unknown.
Other Names for This Condition
- MASLD
- NAFLD
- Non-alcoholic fatty liver disease
- Non-alcoholic steatohepatitis
Additional Information & Resources
Genetic Testing Information
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Ajmera V, Cepin S, Tesfai K, Hofflich H, Cadman K, Lopez S, Madamba E, Bettencourt R, Richards L, Behling C, Sirlin CB, Loomba R. A prospective study on the prevalence of NAFLD, advanced fibrosis, cirrhosis and hepatocellular carcinoma in people with type 2 diabetes. J Hepatol. 2023 Mar;78(3):471-478. doi: 10.1016/j.jhep.2022.11.010. Epub 2022 Nov 19. Citation on PubMed
- Eslam M, Sanyal AJ, George J; International Consensus Panel. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology. 2020 May;158(7):1999-2014.e1. doi: 10.1053/j.gastro.2019.11.312. Epub 2020 Feb 8. Citation on PubMed
- Huang DQ, Wong VWS, Rinella ME, Boursier J, Lazarus JV, Yki-Jarvinen H, Loomba R. Metabolic dysfunction-associated steatotic liver disease in adults. Nat Rev Dis Primers. 2025 Mar 6;11(1):14. doi: 10.1038/s41572-025-00599-1. Citation on PubMed
- Kahali B, Halligan B, Speliotes EK. Insights from Genome-Wide Association Analyses of Nonalcoholic Fatty Liver Disease. Semin Liver Dis. 2015 Nov;35(4):375-91. doi: 10.1055/s-0035-1567870. Epub 2015 Dec 16. Citation on PubMed or Free article on PubMed Central
- Krawczyk M, Portincasa P, Lammert F. PNPLA3-associated steatohepatitis: toward a gene-based classification of fatty liver disease. Semin Liver Dis. 2013 Nov;33(4):369-79. doi: 10.1055/s-0033-1358525. Epub 2013 Nov 12. Citation on PubMed
- Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, Romero D, Abdelmalek MF, Anstee QM, Arab JP, Arrese M, Bataller R, Beuers U, Boursier J, Bugianesi E, Byrne CD, Narro GEC, Chowdhury A, Cortez-Pinto H, Cryer DR, Cusi K, El-Kassas M, Klein S, Eskridge W, Fan J, Gawrieh S, Guy CD, Harrison SA, Kim SU, Koot BG, Korenjak M, Kowdley KV, Lacaille F, Loomba R, Mitchell-Thain R, Morgan TR, Powell EE, Roden M, Romero-Gomez M, Silva M, Singh SP, Sookoian SC, Spearman CW, Tiniakos D, Valenti L, Vos MB, Wong VW, Xanthakos S, Yilmaz Y, Younossi Z, Hobbs A, Villota-Rivas M, Newsome PN; NAFLD Nomenclature consensus group. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Ann Hepatol. 2024 Jan-Feb;29(1):101133. doi: 10.1016/j.aohep.2023.101133. Epub 2023 Jun 24. Citation on PubMed
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, Kleiner DE, Loomba R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023 May 1;77(5):1797-1835. doi: 10.1097/HEP.0000000000000323. Epub 2023 Mar 17. No abstract available. Citation on PubMed
- Seko Y, Yamaguchi K, Shima T, Iwaki M, Takahashi H, Kawanaka M, Tanaka S, Mitsumoto Y, Yoneda M, Nakajima A, Okanoue T, Itoh Y. Clinical Utility of Genetic Variants in PNPLA3 and TM6SF2 to Predict Liver-Related Events in Metabolic Dysfunction-Associated Steatotic Liver Disease. Liver Int. 2025 Apr;45(4):e16124. doi: 10.1111/liv.16124. Epub 2024 Oct 7. Citation on PubMed
- Severson TJ, Besur S, Bonkovsky HL. Genetic factors that affect nonalcoholic fatty liver disease: A systematic clinical review. World J Gastroenterol. 2016 Aug 7;22(29):6742-56. doi: 10.3748/wjg.v22.i29.6742. Citation on PubMed or Free article on PubMed Central
- Yu J, Marsh S, Hu J, Feng W, Wu C. The Pathogenesis of Nonalcoholic Fatty Liver Disease: Interplay between Diet, Gut Microbiota, and Genetic Background. Gastroenterol Res Pract. 2016;2016:2862173. doi: 10.1155/2016/2862173. Epub 2016 May 9. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.