

Description
Megacystis-microcolon-intestinal hypoperistalsis syndrome (MMIHS) is a severe disorder affecting the muscles that line the bladder and intestines. It is characterized by impairment of the muscle contractions that move food through the digestive tract (peristalsis) and empty the bladder.
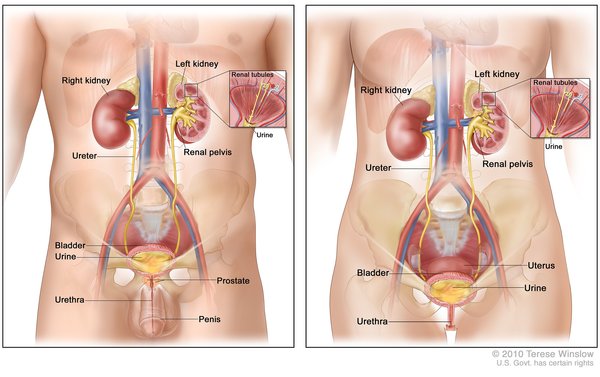
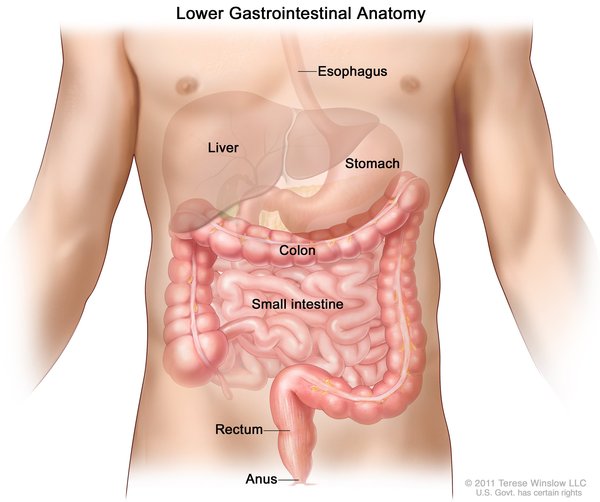
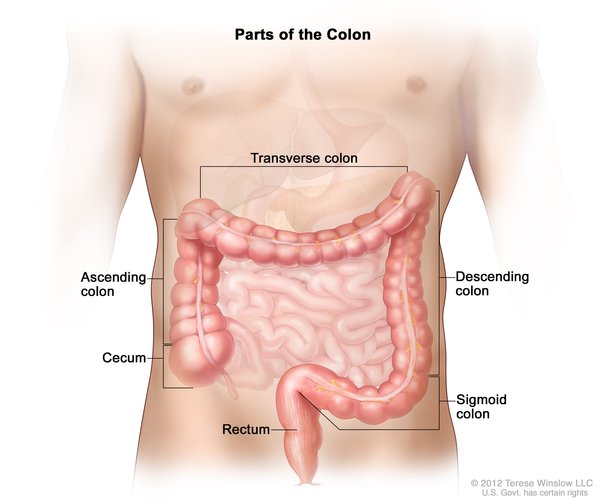
Some of the major features of MMIHS can be recognized before birth using ultrasound imaging. Affected fetuses have an enlarged bladder (megacystis) because it does not empty. In addition, the large intestine (colon) is abnormally narrow (microcolon) because of a shortage of functional muscle lining it. Intestinal and bladder problems persist throughout life.
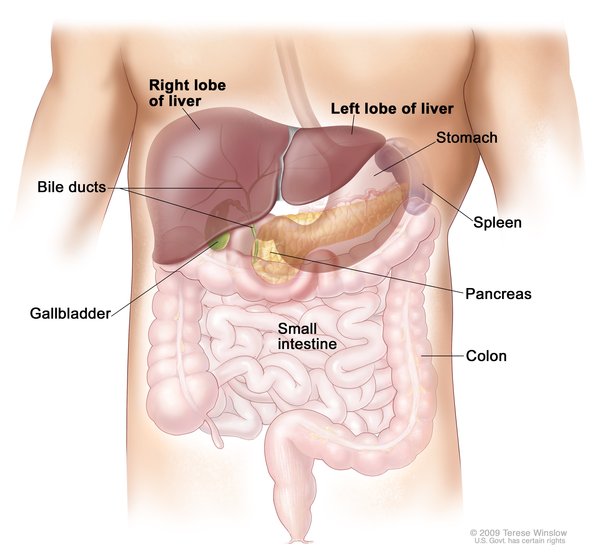
After birth, the continued impairment of peristalsis (hypoperistalsis) often causes a digestive condition called intestinal pseudo-obstruction. This condition, which mimics a physical blockage (obstruction) of the intestines but without an actual blockage, leads to a buildup of partially digested food in the intestines. This buildup can cause abdominal swelling (distention) and pain, nausea, and vomiting. The vomit usually contains a green or yellow digestive fluid called bile. Because digestion is impeded and the body does not get the nutrients from food, nutritional support is usually needed, which is given through intravenous feedings (parenteral nutrition). While some affected individuals rely solely on intravenous feedings, others require it only on occasion. Long-term use of parenteral nutrition can lead to liver problems.
The reduced ability to pass urine also contributes to painful distention of the abdomen. Many people with MMIHS require placement of a tube (urinary catheter) to remove urine from the bladder.
Another abnormality in some people with MMIHS is intestinal malrotation, in which the intestines do not fold properly. Instead, they twist abnormally, often causing a blockage. Individuals with MMIHS can also develop problems with the kidneys or the ureters, which are the ducts that carry urine from the kidneys to the bladder.
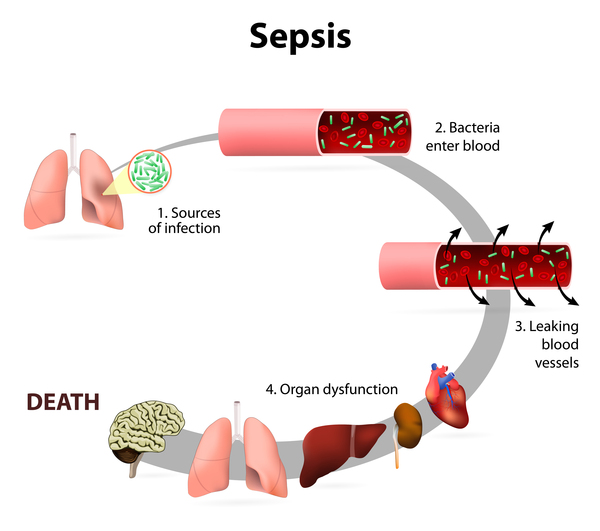
The life expectancy of people with MMIHS is shorter than normal, often due to malnutrition, overwhelming infection (sepsis), or the failure of multiple organs.
Frequency
MMIHS is a rare disorder. More than 200 cases have been reported in the medical literature.
Causes
MMIHS can be caused by mutations in one of several genes, the most studied of which is ACTG2. The ACTG2 gene provides instructions for making a protein called gamma (γ)-2 actin. The γ-2 actin proteins organize into filaments that are important for the tensing of muscle fibers (muscle contraction), specifically contraction of smooth muscles of the urinary and intestinal tracts. These contractions empty urine from the bladder and move food through the intestines.
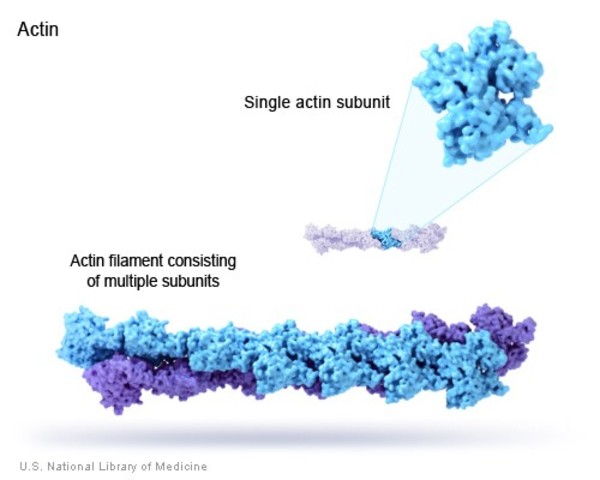
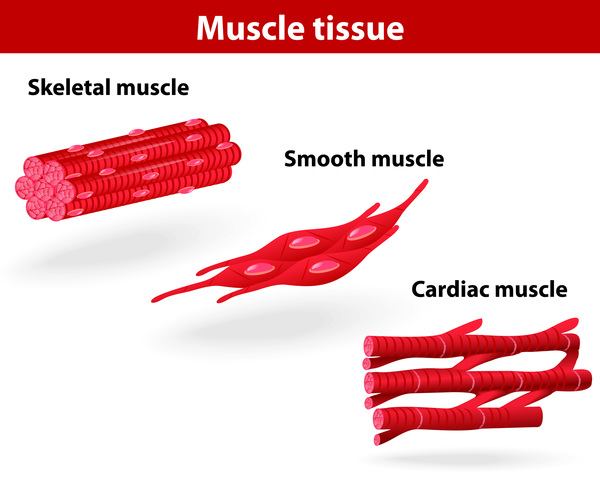
ACTG2 gene mutations lead to production of an altered γ-2 actin protein. These changes hinder the formation of actin filaments, which impairs the ability of smooth muscle in the bladder and intestines to contract. These problems with muscle contractions impair the release of urine and the movement of food through the intestines, leading to the key features of MMIHS.
Mutations in other genes have been found to cause rare cases of MMIHS. The proteins produced from these genes are also involved in smooth muscle contraction. Approximately 10 percent of people with MMIHS do not have a mutation in one of the identified genes. It is likely that additional genes that have not been identified are also involved in the disorder.
Inheritance
When caused by ACTG2 gene mutations, MMIHS follows an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. These cases result from new (de novo) mutations in the gene that occur during the formation of reproductive cells (eggs or sperm) or in early embryonic development. In these cases, affected individuals have no history of the disorder in their family.

When caused by mutations in other identified genes, MMIHS is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.

Other Names for This Condition
- Berdon syndrome
- Megacystis, microcolon, hypoperistalsis syndrome
- MMIH syndrome
- MMIHS
Additional Information & Resources
Genetic Testing Information
- Genetic Testing Registry: Megacystis-microcolon-intestinal hypoperistalsis syndrome 1

- Genetic Testing Registry: Megacystis-microcolon-intestinal hypoperistalsis syndrome 2
- Genetic Testing Registry: Megacystis-microcolon-intestinal hypoperistalsis syndrome 3
- Genetic Testing Registry: Megacystis-microcolon-intestinal hypoperistalsis syndrome 5
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Bhagwat PK, Wangler MF. ACTG2 Visceral Myopathy. 2015 Jun 11 [updated 2021 May 6]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK299311/ Citation on PubMed
- Gauthier J, Ouled Amar Bencheikh B, Hamdan FF, Harrison SM, Baker LA, Couture F, Thiffault I, Ouazzani R, Samuels ME, Mitchell GA, Rouleau GA, Michaud JL, Soucy JF. A homozygous loss-of-function variant in MYH11 in a case with megacystis-microcolon-intestinal hypoperistalsis syndrome. Eur J Hum Genet. 2015 Sep;23(9):1266-8. doi: 10.1038/ejhg.2014.256. Epub 2014 Nov 19. Citation on PubMed or Free article on PubMed Central
- Halim D, Brosens E, Muller F, Wangler MF, Beaudet AL, Lupski JR, Akdemir ZHC, Doukas M, Stoop HJ, de Graaf BM, Brouwer RWW, van Ijcken WFJ, Oury JF, Rosenblatt J, Burns AJ, Tibboel D, Hofstra RMW, Alves MM. Loss-of-Function Variants in MYLK Cause Recessive Megacystis Microcolon Intestinal Hypoperistalsis Syndrome. Am J Hum Genet. 2017 Jul 6;101(1):123-129. doi: 10.1016/j.ajhg.2017.05.011. Epub 2017 Jun 8. Citation on PubMed or Free article on PubMed Central
- Halim D, Hofstra RM, Signorile L, Verdijk RM, van der Werf CS, Sribudiani Y, Brouwer RW, van IJcken WF, Dahl N, Verheij JB, Baumann C, Kerner J, van Bever Y, Galjart N, Wijnen RM, Tibboel D, Burns AJ, Muller F, Brooks AS, Alves MM. ACTG2 variants impair actin polymerization in sporadic Megacystis Microcolon Intestinal Hypoperistalsis Syndrome. Hum Mol Genet. 2016 Feb 1;25(3):571-83. doi: 10.1093/hmg/ddv497. Epub 2015 Dec 8. Citation on PubMed
- Halim D, Wilson MP, Oliver D, Brosens E, Verheij JB, Han Y, Nanda V, Lyu Q, Doukas M, Stoop H, Brouwer RW, van IJcken WF, Slivano OJ, Burns AJ, Christie CK, de Mesy Bentley KL, Brooks AS, Tibboel D, Xu S, Jin ZG, Djuwantono T, Yan W, Alves MM, Hofstra RM, Miano JM. Loss of LMOD1 impairs smooth muscle cytocontractility and causes megacystis microcolon intestinal hypoperistalsis syndrome in humans and mice. Proc Natl Acad Sci U S A. 2017 Mar 28;114(13):E2739-E2747. doi: 10.1073/pnas.1620507114. Epub 2017 Mar 14. Citation on PubMed or Free article on PubMed Central
- Thorson W, Diaz-Horta O, Foster J 2nd, Spiliopoulos M, Quintero R, Farooq A, Blanton S, Tekin M. De novo ACTG2 mutations cause congenital distended bladder, microcolon, and intestinal hypoperistalsis. Hum Genet. 2014 Jun;133(6):737-42. doi: 10.1007/s00439-013-1406-0. Epub 2013 Dec 13. Citation on PubMed
- Wangler MF, Gonzaga-Jauregui C, Gambin T, Penney S, Moss T, Chopra A, Probst FJ, Xia F, Yang Y, Werlin S, Eglite I, Kornejeva L, Bacino CA, Baldridge D, Neul J, Lehman EL, Larson A, Beuten J, Muzny DM, Jhangiani S; Baylor-Hopkins Center for Mendelian Genomics; Gibbs RA, Lupski JR, Beaudet A. Heterozygous de novo and inherited mutations in the smooth muscle actin (ACTG2) gene underlie megacystis-microcolon-intestinal hypoperistalsis syndrome. PLoS Genet. 2014 Mar 27;10(3):e1004258. doi: 10.1371/journal.pgen.1004258. eCollection 2014 Mar. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.