

Description
An epidermal nevus (plural: nevi) is an abnormal, noncancerous (benign) patch of skin caused by an overgrowth of cells in the outermost layer of skin (epidermis). Epidermal nevi are typically seen at birth or develop in early childhood. Affected individuals have one or more nevi that vary in size.
There are several types of epidermal nevus that are defined in part by the type of epidermal cell involved. The epidermis is composed primarily of a specific cell type called a keratinocyte. One group of epidermal nevi, called keratinocytic or nonorganoid epidermal nevi, includes nevi that involve only keratinocytes. Keratinocytic epidermal nevi are typically found on the torso or limbs. They can be flat, tan or brown patches of skin or raised, velvety patches. As affected individuals age, the nevi can become thicker and darker and develop a wart-like (verrucous) appearance. Often, keratinocytic epidermal nevi follow a pattern on the skin known as the lines of Blaschko. The lines of Blaschko, which are normally invisible on skin, are thought to follow the paths along which cells migrate as the skin develops before birth. Keratinocytic epidermal nevi are also known as linear epidermal nevi or verrucous epidermal nevi, based on characteristics of their appearance.
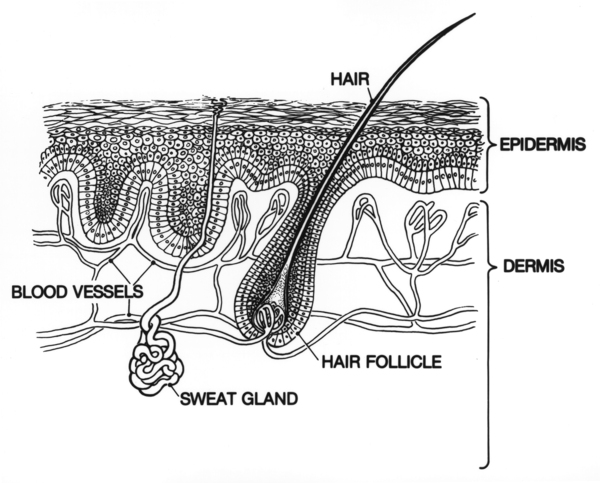
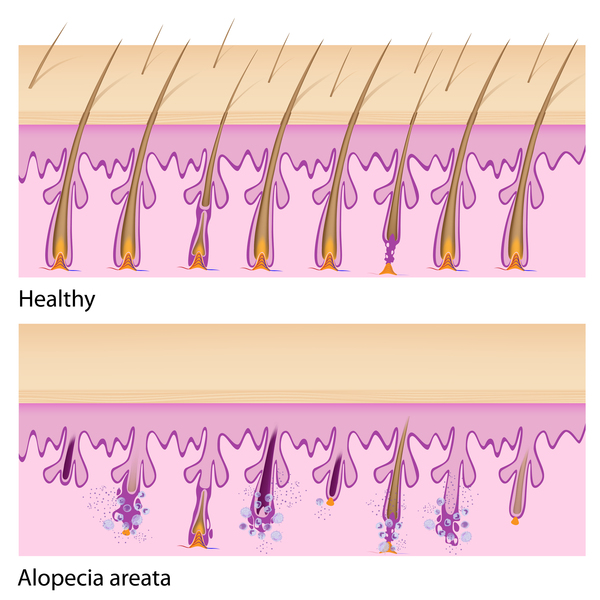
Other types of epidermal nevi involve additional types of epidermal cells, such as the cells that make up the hair follicles, the sweat glands, or the sebaceous glands (glands in the skin that produce a substance that protects the skin and hair). These nevi comprise a group called organoid epidermal nevi. A common type of organoid epidermal nevus is called nevus sebaceous. Nevi in this group are waxy, yellow-orange patches of skin, usually on the scalp or face. The patch is typically hairless, leaving a distinct region of baldness (alopecia). Similar to keratinocytic epidermal nevi, nevi sebaceous can become thicker and more verrucous over time. In about one-quarter of people with a nevus sebaceous, a tumor forms in the same region as the nevus. The tumor is usually benign, although rarely cancerous (malignant) tumors develop.
Some affected individuals have only an epidermal nevus and no other abnormalities. However, sometimes people with an epidermal nevus also have problems in other body systems, such as the brain, eyes, or bones. In these cases, the affected individual has a condition called an epidermal nevus syndrome. There are several different epidermal nevus syndromes characterized by the type of epidermal nevus involved.
Frequency
Epidermal nevi are estimated to occur in 1 to 3 in 1,000 people.
Causes
Several genes have been associated with different types of epidermal nevus. Mutations in the FGFR3 gene and PIK3CA gene account for about forty percent of keratinocytic epidermal nevi. Mutations in the HRAS gene are found in a majority of people with a nevus sebaceous and are also associated with keratinocytic epidermal nevi. Genes related to HRAS (called KRAS and NRAS) are less commonly involved in nevi sebaceous or keratinocytic epidermal nevi. Other genes, some of which have not been identified, are also involved in epidermal nevi.
FGFR3, PIK3CA, HRAS, and other related RAS genes provide instructions for making proteins that are involved in cellular signaling. This signaling helps direct several important cellular processes, including regulation of growth and division of skin cells. In order to relay signals, the proteins must be turned on (activated), which triggers a cascade of chemical reactions inside the cell that control growth and other cellular functions.
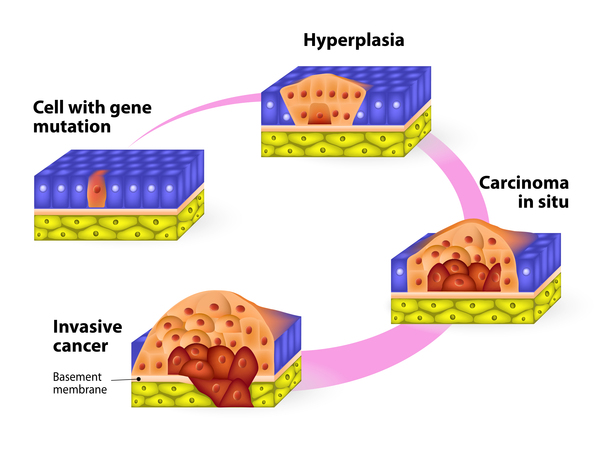
Mutations in the genes mentioned above lead to proteins that are constantly turned on. Studies suggest that cells with a mutation in one of these genes grow and divide more than normal cells. This uncontrolled cell division results in overgrowth of skin cells, leading to epidermal nevi.
Mutations associated with an epidermal nevus are present only in the cells of the nevus, not in the normal skin cells surrounding it. Because the mutation is found in some of the body's cells but not in others, people with an epidermal nevus are said to be mosaic for the mutation.
Inheritance
This condition is generally not inherited but arises from mutations in the body's cells that occur after conception. This type of alteration is called a somatic mutation.
Occasionally, a somatic FGFR3 gene mutation occurs in an affected parent's reproductive cells (sperm or eggs) and is passed to the next generation. When this occurs, the gene mutation is found in every cell in the child's body, which results in skeletal abnormalities rather than epidermal nevus.
Other Names for This Condition
- Epidermal naevus
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Brandling-Bennett HA, Morel KD. Epidermal nevi. Pediatr Clin North Am. 2010 Oct;57(5):1177-98. doi: 10.1016/j.pcl.2010.07.004. Citation on PubMed
- Groesser L, Herschberger E, Ruetten A, Ruivenkamp C, Lopriore E, Zutt M, Langmann T, Singer S, Klingseisen L, Schneider-Brachert W, Toll A, Real FX, Landthaler M, Hafner C. Postzygotic HRAS and KRAS mutations cause nevus sebaceous and Schimmelpenning syndrome. Nat Genet. 2012 Jun 10;44(7):783-7. doi: 10.1038/ng.2316. Citation on PubMed
- Hafner C, Di Martino E, Pitt E, Stempfl T, Tomlinson D, Hartmann A, Landthaler M, Knowles M, Vogt T. FGFR3 mutation affects cell growth, apoptosis and attachment in keratinocytes. Exp Cell Res. 2010 Jul 15;316(12):2008-16. doi: 10.1016/j.yexcr.2010.04.021. Epub 2010 Apr 24. Citation on PubMed
- Hafner C, Lopez-Knowles E, Luis NM, Toll A, Baselga E, Fernandez-Casado A, Hernandez S, Ribe A, Mentzel T, Stoehr R, Hofstaedter F, Landthaler M, Vogt T, Pujol RM, Hartmann A, Real FX. Oncogenic PIK3CA mutations occur in epidermal nevi and seborrheic keratoses with a characteristic mutation pattern. Proc Natl Acad Sci U S A. 2007 Aug 14;104(33):13450-4. doi: 10.1073/pnas.0705218104. Epub 2007 Aug 2. Citation on PubMed or Free article on PubMed Central
- Hafner C, Toll A, Gantner S, Mauerer A, Lurkin I, Acquadro F, Fernandez-Casado A, Zwarthoff EC, Dietmaier W, Baselga E, Parera E, Vicente A, Casanova A, Cigudosa J, Mentzel T, Pujol RM, Landthaler M, Real FX. Keratinocytic epidermal nevi are associated with mosaic RAS mutations. J Med Genet. 2012 Apr;49(4):249-53. doi: 10.1136/jmedgenet-2011-100637. Citation on PubMed
- Hafner C, van Oers JM, Vogt T, Landthaler M, Stoehr R, Blaszyk H, Hofstaedter F, Zwarthoff EC, Hartmann A. Mosaicism of activating FGFR3 mutations in human skin causes epidermal nevi. J Clin Invest. 2006 Aug;116(8):2201-2207. doi: 10.1172/JCI28163. Citation on PubMed or Free article on PubMed Central
- Hernandez S, Toll A, Baselga E, Ribe A, Azua-Romeo J, Pujol RM, Real FX. Fibroblast growth factor receptor 3 mutations in epidermal nevi and associated low grade bladder tumors. J Invest Dermatol. 2007 Jul;127(7):1664-6. doi: 10.1038/sj.jid.5700705. Epub 2007 Jan 25. Citation on PubMed
- Miranda LQ, Fracaroli TS, Fonseca JC, Fontenelle E, Curvo RP, Porto LC, Souto R. Analysis of mutations in the PIK3CA and FGFR3 genes in verrucous epidermal nevus. An Bras Dermatol. 2013 Nov-Dec;88(6 Suppl 1):36-8. doi: 10.1590/abd1806-4841.20132055. Citation on PubMed or Free article on PubMed Central
- Toll A, Fernandez LC, Pons T, Groesser L, Sagrera A, Carrillo-de Santa Pau E, Vicente A, Baselga E, Vazquez M, Beltran S, Pisano DG, Rueda D, Gut M, Pujol RM, Hafner C, Gut I, Valencia A, Real FX. Somatic Embryonic FGFR2 Mutations in Keratinocytic Epidermal Nevi. J Invest Dermatol. 2016 Aug;136(8):1718-1721. doi: 10.1016/j.jid.2016.03.040. Epub 2016 Apr 19. No abstract available. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.