

Description
Congenital dyserythropoietic anemia (CDA) is a rare group of inherited blood disorders that affects the development of red blood cells. In people with CDA, immature red blood cells do not develop into normal, mature cells. As a result, affected individuals have a significant reduction in the number of functional red blood cells (anemia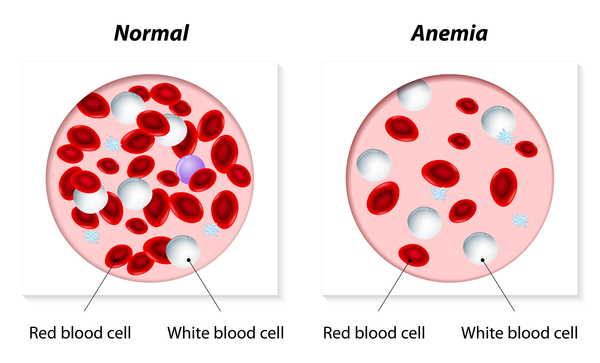 ). The term "dyserythropoietic" refers to the abnormal red blood cell shape that occurs in people with this condition. People with CDA typically have mild to moderate anemia. In some cases, affected individuals have severe anemia that may require frequent blood transfusions to replenish the supply of red blood cells.
). The term "dyserythropoietic" refers to the abnormal red blood cell shape that occurs in people with this condition. People with CDA typically have mild to moderate anemia. In some cases, affected individuals have severe anemia that may require frequent blood transfusions to replenish the supply of red blood cells.
The signs and symptoms of CDA can include tiredness (fatigue), weakness, yellowing of the skin and eyes (jaundice), and an enlarged liver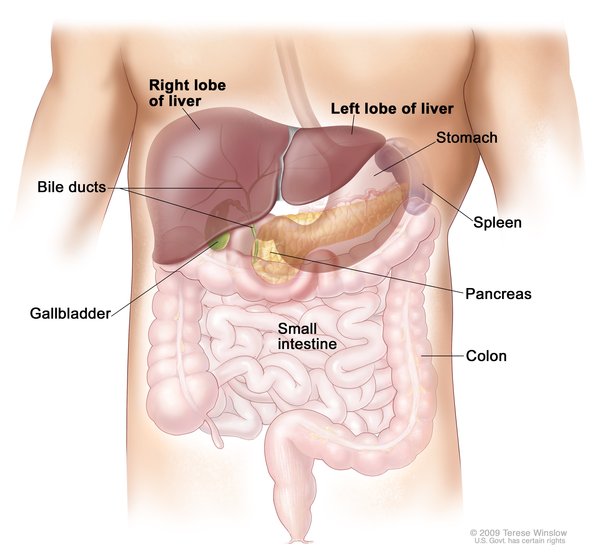 and spleen (hepatosplenomegaly). CDA also causes the body to absorb too much iron (iron overload), which can damage tissues and organs.
and spleen (hepatosplenomegaly). CDA also causes the body to absorb too much iron (iron overload), which can damage tissues and organs.
There are multiple types of CDA. Each type has a different genetic cause and distinct but overlapping patterns of signs and symptoms.
CDA type I is characterized by moderate to severe anemia that typically begins in childhood or adolescence, although the condition can be detected before birth in some cases. In addition to the signs and symptoms common to all types of CDA, individuals with CDA type I can have skeletal issues, including short stature or abnormalities of the fingers or toes.
The anemia associated with CDA type II can range from mild to severe, and it usually develops in adolescence or early adulthood. Individuals with CDA type II may develop hard deposits in the gallbladder called gallstones in addition to the usual signs and symptoms of CDA.
called gallstones in addition to the usual signs and symptoms of CDA.
CDA type III can result in anemia that ranges from mild to severe, depending on the genetic cause, and typically begins in infancy or childhood. Some people with CDA type III do not receive a diagnosis until later in life because they have very mild symptoms. In some cases, individuals with CDA type III develop a blood disorder known as monoclonal gammopathy, which can lead to a cancer of white blood cells (multiple myeloma). Some people with CDA type III have eye abnormalities that can cause vision impairment.
CDA type IV is characterized by moderate to severe anemia that typically develops early in life, although the condition can be detected before birth in some cases. Affected individuals can have extensive swelling caused by fluid accumulation before birth (hydrops fetalis). In addition to the signs and symptoms that are common to all types of CDA, individuals with CDA type IV often have short stature.
Frequency
CDA is a rare disorder, though the exact prevalence of CDA is unknown. CDA type II is the most common form of the disorder. Because CDA is rare and the signs and symptoms may be mild or overlap with those of other disorders, many cases likely remain undiagnosed or are incorrectly diagnosed as other disorders.
Causes
Variants (also called mutations) in multiple genes have been found to cause CDA. Variants in these genes cause CDA by disrupting the normal development of red blood cells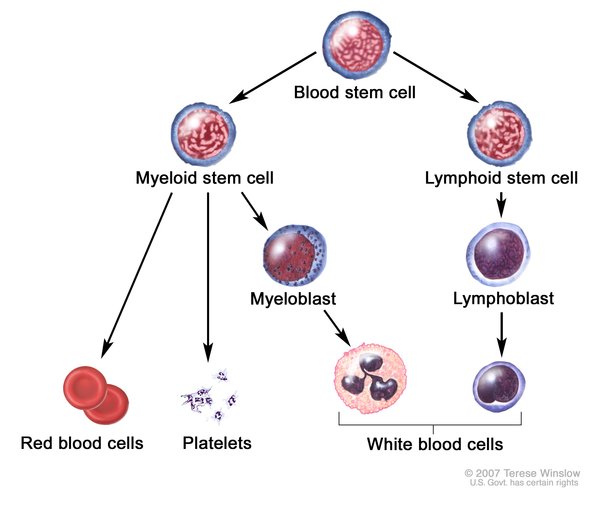 (erythropoiesis). In people with CDA, immature red blood cells called erythroblasts are unusually shaped and have other abnormalities. These abnormal erythroblasts either develop into irregular red blood cells or do not develop at all. Irregular red blood cells are quickly removed from circulation. The cells go to the spleen for destruction, and the resulting iron goes to the liver to be processed. The overall shortage of healthy red blood cells leads to the characteristic signs and symptoms of CDA, including anemia, hepatosplenomegaly, and iron overload.
(erythropoiesis). In people with CDA, immature red blood cells called erythroblasts are unusually shaped and have other abnormalities. These abnormal erythroblasts either develop into irregular red blood cells or do not develop at all. Irregular red blood cells are quickly removed from circulation. The cells go to the spleen for destruction, and the resulting iron goes to the liver to be processed. The overall shortage of healthy red blood cells leads to the characteristic signs and symptoms of CDA, including anemia, hepatosplenomegaly, and iron overload.
CDA type I is caused by variants in the CDAN1 or CDIN1 gene. These genes provide instructions for making proteins that can attach (bind) to each other and play roles in cell division and erythropoiesis. In at least 10 percent of cases of CDA type I, the cause of the condition is unknown.
CDA type II is caused by variants in the SEC23B gene. This gene provides instructions for making a protein that is involved in the transport of other proteins within cells. During erythropoiesis, this protein may help ensure that proteins are transported to the areas where they are needed.
CDA type III is caused by variants in either the KIF23 or RACGAP1 gene. The KIF23 and RACGAP1 genes provides instructions for making proteins that can bind to each other to form a complex. This complex plays a critical role in the step of cell division in which the dividing cells separate from one another (cytokinesis). The complex also appears to be particularly important in the bone marrow where red blood cells grow and divide (proliferate).
CDA type IV is caused by variants in the KLF1 gene. This gene provides instructions for making a protein that regulates the activity of genes involved in erythropoiesis.
Inheritance
The inheritance pattern of CDA depends on the type of the disorder. CDA types I and II are inherited in an autosomal recessive pattern , which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition. When CDA type III is caused by variants in the RACGAP1 gene, it is also inherited in an autosomal recessive pattern.
, which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition. When CDA type III is caused by variants in the RACGAP1 gene, it is also inherited in an autosomal recessive pattern.
CDA type IV appears to have an autosomal dominant pattern of inheritance. Autosomal dominant inheritance means that one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases, an affected person has one parent with the condition. When CDA type III is caused by variants in the KIF23 gene, it is also inherited in an autosomal dominant pattern.
of inheritance. Autosomal dominant inheritance means that one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases, an affected person has one parent with the condition. When CDA type III is caused by variants in the KIF23 gene, it is also inherited in an autosomal dominant pattern.
Other Names for This Condition
- Anemia, dyserythropoietic, congenital
- CDA
- congenital dyserythropoietic anaemia
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
- ANEMIA, CONGENITAL DYSERYTHROPOIETIC, TYPE Ia; CDAN1A
- ANEMIA, CONGENITAL DYSERYTHROPOIETIC, TYPE Ib; CDAN1B
- ANEMIA, CONGENITAL DYSERYTHROPOIETIC, TYPE II; CDAN2
- ANEMIA, CONGENITAL DYSERYTHROPOIETIC, TYPE IIIa; CDAN3A
- ANEMIA, CONGENITAL DYSERYTHROPOIETIC, TYPE IIIb, AUTOSOMAL RECESSIVE; CDAN3B
- ANEMIA, CONGENITAL DYSERYTHROPOIETIC, TYPE IVa; CDAN4A
Scientific Articles on PubMed
References
- Denecke J, Marquardt T. Congenital dyserythropoietic anemia type II (CDAII/HEMPAS): where are we now? Biochim Biophys Acta. 2009 Sep;1792(9):915-20. doi: 10.1016/j.bbadis.2008.12.005. Epub 2008 Dec 25. Citation on PubMed
- Dgany O, Avidan N, Delaunay J, Krasnov T, Shalmon L, Shalev H, Eidelitz-Markus T, Kapelushnik J, Cattan D, Pariente A, Tulliez M, Cretien A, Schischmanoff PO, Iolascon A, Fibach E, Koren A, Rossler J, Le Merrer M, Yaniv I, Zaizov R, Ben-Asher E, Olender T, Lancet D, Beckmann JS, Tamary H. Congenital dyserythropoietic anemia type I is caused by mutations in codanin-1. Am J Hum Genet. 2002 Dec;71(6):1467-74. doi: 10.1086/344781. Epub 2002 Nov 14. Citation on PubMed or Free article on PubMed Central
- Heimpel H, Anselstetter V, Chrobak L, Denecke J, Einsiedler B, Gallmeier K, Griesshammer A, Marquardt T, Janka-Schaub G, Kron M, Kohne E. Congenital dyserythropoietic anemia type II: epidemiology, clinical appearance, and prognosis based on long-term observation. Blood. 2003 Dec 15;102(13):4576-81. doi: 10.1182/blood-2003-02-0613. Epub 2003 Aug 21. Citation on PubMed
- Heimpel H, Schwarz K, Ebnother M, Goede JS, Heydrich D, Kamp T, Plaumann L, Rath B, Roessler J, Schildknecht O, Schmid M, Wuillemin W, Einsiedler B, Leichtle R, Tamary H, Kohne E. Congenital dyserythropoietic anemia type I (CDA I): molecular genetics, clinical appearance, and prognosis based on long-term observation. Blood. 2006 Jan 1;107(1):334-40. doi: 10.1182/blood-2005-01-0421. Epub 2005 Sep 1. Citation on PubMed
- Heimpel H. Congenital dyserythropoietic anemias: epidemiology, clinical significance, and progress in understanding their pathogenesis. Ann Hematol. 2004 Oct;83(10):613-21. doi: 10.1007/s00277-004-0892-5. Epub 2004 Jul 20. Citation on PubMed
- Iolascon A, Andolfo I, Russo R. Congenital dyserythropoietic anemias. Blood. 2020 Sep 10;136(11):1274-1283. doi: 10.1182/blood.2019000948. Citation on PubMed
- Olijnik AA, Roy NBA, Scott C, Marsh JA, Brown J, Lauschke K, Ask K, Roberts N, Downes DJ, Brolih S, Johnson E, Xella B, Proven M, Hipkiss R, Ryan K, Frisk P, Makk J, Stattin EM, Sadasivam N, McIlwaine L, Hill QA, Renella R, Hughes JR, Gibbons RJ, Groth A, McHugh PJ, Higgs DR, Buckle VJ, Babbs C. Genetic and functional insights into CDA-I prevalence and pathogenesis. J Med Genet. 2021 Mar;58(3):185-195. doi: 10.1136/jmedgenet-2020-106880. Epub 2020 Jun 9. Citation on PubMed
- Renella R, Wood WG. The congenital dyserythropoietic anemias. Hematol Oncol Clin North Am. 2009 Apr;23(2):283-306. doi: 10.1016/j.hoc.2009.01.010. Citation on PubMed
- Russo R, Iolascon A, Andolfo I, Marra R, Rosato BE. Updates on clinical and laboratory aspects of hereditary dyserythropoietic anemias. Int J Lab Hematol. 2024 Aug;46(4):595-605. doi: 10.1111/ijlh.14307. Epub 2024 May 15. Citation on PubMed
- Russo R, Marra R, Andolfo I, De Rosa G, Rosato BE, Manna F, Gambale A, Raia M, Unal S, Barella S, Iolascon A. Characterization of Two Cases of Congenital Dyserythropoietic Anemia Type I Shed Light on the Uncharacterized C15orf41 Protein. Front Physiol. 2019 May 22;10:621. doi: 10.3389/fphys.2019.00621. eCollection 2019. Citation on PubMed
- Sandstrom H, Wahlin A. Congenital dyserythropoietic anemia type III. Haematologica. 2000 Jul;85(7):753-7. Citation on PubMed
- Schwarz K, Iolascon A, Verissimo F, Trede NS, Horsley W, Chen W, Paw BH, Hopfner KP, Holzmann K, Russo R, Esposito MR, Spano D, De Falco L, Heinrich K, Joggerst B, Rojewski MT, Perrotta S, Denecke J, Pannicke U, Delaunay J, Pepperkok R, Heimpel H. Mutations affecting the secretory COPII coat component SEC23B cause congenital dyserythropoietic anemia type II. Nat Genet. 2009 Aug;41(8):936-40. doi: 10.1038/ng.405. Epub 2009 Jun 28. Citation on PubMed
- Tamary H, Dgany O, Proust A, Krasnov T, Avidan N, Eidelitz-Markus T, Tchernia G, Genevieve D, Cormier-Daire V, Bader-Meunier B, Ferrero-Vacher C, Munzer M, Gruppo R, Fibach E, Konen O, Yaniv I, Delaunay J. Clinical and molecular variability in congenital dyserythropoietic anaemia type I. Br J Haematol. 2005 Aug;130(4):628-34. doi: 10.1111/j.1365-2141.2005.05642.x. Citation on PubMed
- Tamary H, Dgany O. Congenital Dyserythropoietic Anemia Type I. 2009 Apr 21 [updated 2021 Jul 29]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK5313/ Citation on PubMed
- Wickramasinghe SN, Wood WG. Advances in the understanding of the congenital dyserythropoietic anaemias. Br J Haematol. 2005 Nov;131(4):431-46. doi: 10.1111/j.1365-2141.2005.05757.x. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.