

Description
Achondroplasia is the most common form of short-limbed dwarfism. The word achondroplasia means "without cartilage formation." Cartilage is a tough but flexible tissue that makes up much of the skeleton during early development. However, in people with achondroplasia the problem is not forming cartilage but converting it to bone (a process called ossification), particularly in the long bones of the arms and legs. Achondroplasia is similar to another skeletal disorder called hypochondroplasia, but the features of achondroplasia tend to be more severe.
All people with achondroplasia have short stature. Without treatment, the average height of an adult male with achondroplasia is 131 centimeters (4 feet, 4 inches), and the average height for adult females is 124 centimeters (4 feet, 1 inch). Characteristic features of achondroplasia include an average-size trunk, short arms and legs with particularly short upper arms and thighs, limited range of motion at the elbows, and an enlarged head (macrocephaly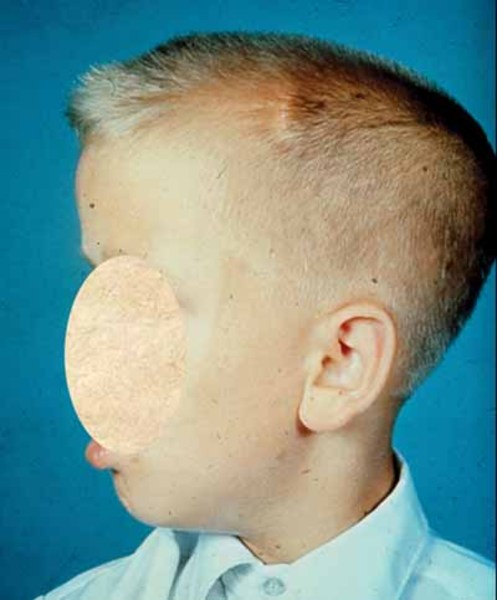 ) with a prominent forehead
) with a prominent forehead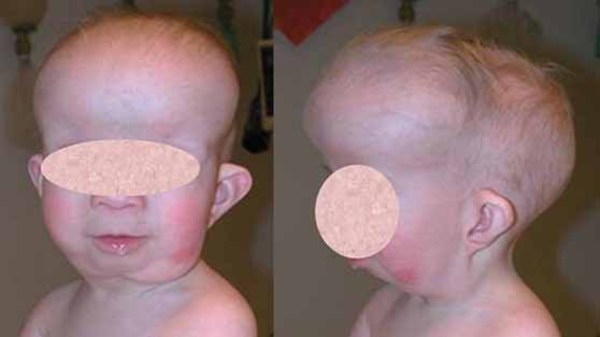 . Fingers are typically short and the ring finger and middle finger may diverge, giving the hand a three-pronged (trident
. Fingers are typically short and the ring finger and middle finger may diverge, giving the hand a three-pronged (trident ) appearance.
) appearance.
Health problems commonly associated with achondroplasia include obesity and recurrent ear infections. People with achondroplasia are generally of normal intelligence. In childhood, individuals with the condition usually develop a pronounced and permanent sway of the lower back (lordosis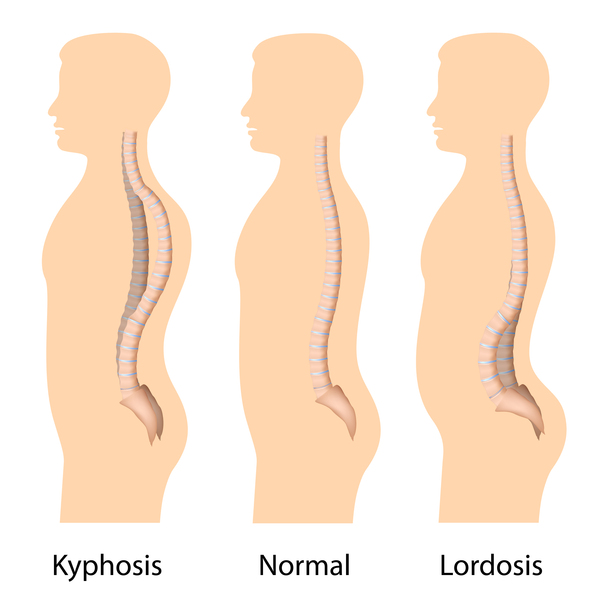 ) and bowed legs. Some affected people also develop abnormal front-to-back curvature of the spine (kyphosis
) and bowed legs. Some affected people also develop abnormal front-to-back curvature of the spine (kyphosis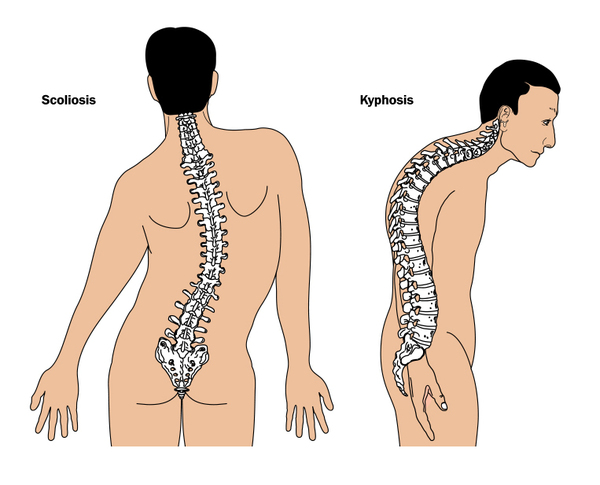 ) and back pain.
) and back pain.
As affected individuals age, they may experience a potentially serious complication of achondroplasia called spinal stenosis.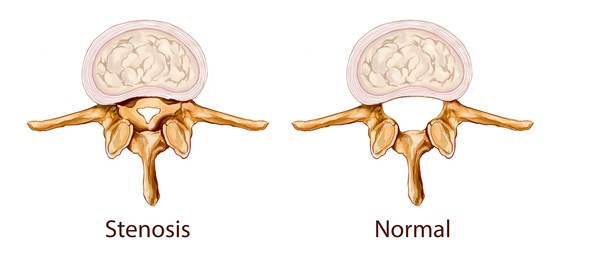 Spinal stenosis is a narrowing of the spinal canal that can pinch (compress) the upper part of the spinal cord. Spinal stenosis causes with pain, tingling, and weakness in the legs that can make walking difficult. An uncommon but serious complication of achondroplasia in early childhood is stenosis of the hole at the base of the skull where the spinal cord comes out of brain (foramen magnum). This complication can cause compression of the brain stem, which can lead to pauses in breathing during sleep (sleep apnea) or a condition known as hydrocephalus. Hydrocephalus is a buildup of fluid in the brain that can lead to increased head size and related brain abnormalities.
Spinal stenosis is a narrowing of the spinal canal that can pinch (compress) the upper part of the spinal cord. Spinal stenosis causes with pain, tingling, and weakness in the legs that can make walking difficult. An uncommon but serious complication of achondroplasia in early childhood is stenosis of the hole at the base of the skull where the spinal cord comes out of brain (foramen magnum). This complication can cause compression of the brain stem, which can lead to pauses in breathing during sleep (sleep apnea) or a condition known as hydrocephalus. Hydrocephalus is a buildup of fluid in the brain that can lead to increased head size and related brain abnormalities.
Frequency
Achondroplasia is the most common type of short-limbed dwarfism. The condition occurs in 1 in 15,000 to 40,000 newborns.
Causes
Variants (also called mutations) in the FGFR3 gene cause achondroplasia. The FGFR3 gene provides instructions for making a protein that is involved in the development and maintenance of bone and brain tissue. Two specific variants in the FGFR3 gene are responsible for almost all cases of achondroplasia. These variants cause the FGFR3 protein to be overly active, which interferes with skeletal development and leads to the disturbances in bone growth seen with this disorder.
Inheritance
Achondroplasia is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. About 80 percent of people with achondroplasia are born to parents who do not have the condition and are of average heights; these cases are caused by new variants in the FGFR3 gene. In the remaining cases, people with achondroplasia inherit an altered FGFR3 gene from one or two affected parents
in the FGFR3 gene. In the remaining cases, people with achondroplasia inherit an altered FGFR3 gene from one or two affected parents .
.
Individuals who inherit two altered copies of the FGFR3 gene typically have a severe form of achondroplasia that causes extreme shortening of the bones and an underdeveloped rib cage. These individuals are usually stillborn or die shortly after birth from respiratory failure.
Other Names for This Condition
- ACH
- Achondroplastic dwarfism
- Dwarf, achondroplastic
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Horton WA, Hall JG, Hecht JT. Achondroplasia. Lancet. 2007 Jul 14;370(9582):162-172. doi: 10.1016/S0140-6736(07)61090-3. Citation on PubMed
- Horton WA, Lunstrum GP. Fibroblast growth factor receptor 3 mutations in achondroplasia and related forms of dwarfism. Rev Endocr Metab Disord. 2002 Dec;3(4):381-5. doi: 10.1023/a:1020914026829. No abstract available. Citation on PubMed
- Horton WA. Recent milestones in achondroplasia research. Am J Med Genet A. 2006 Jan 15;140(2):166-9. doi: 10.1002/ajmg.a.31029. No abstract available. Citation on PubMed
- Laederich MB, Horton WA. Achondroplasia: pathogenesis and implications for future treatment. Curr Opin Pediatr. 2010 Aug;22(4):516-23. doi: 10.1097/MOP.0b013e32833b7a69. Citation on PubMed
- Legare JM, Modaff P. Achondroplasia. 1998 Oct 12 [updated 2026 Apr 9]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1152/ Citation on PubMed
- Savarirayan R, Tofts L, Irving M, Wilcox WR, Bacino CA, Hoover-Fong J, Font RU, Harmatz P, Rutsch F, Bober MB, Polgreen LE, Ginebreda I, Mohnike K, Charrow J, Hoernschemeyer D, Ozono K, Alanay Y, Arundel P, Kotani Y, Yasui N, White KK, Saal HM, Leiva-Gea A, Luna-Gonzalez F, Mochizuki H, Basel D, Porco DM, Jayaram K, Fisheleva E, Huntsman-Labed A, Day JRS. Safe and persistent growth-promoting effects of vosoritide in children with achondroplasia: 2-year results from an open-label, phase 3 extension study. Genet Med. 2021 Dec;23(12):2443-2447. doi: 10.1038/s41436-021-01287-7. Epub 2021 Aug 2. Citation on PubMed
- Trotter TL, Hall JG; American Academy of Pediatrics Committee on Genetics. Health supervision for children with achondroplasia. Pediatrics. 2005 Sep;116(3):771-83. doi: 10.1542/peds.2005-1440. Citation on PubMed
- Vajo Z, Francomano CA, Wilkin DJ. The molecular and genetic basis of fibroblast growth factor receptor 3 disorders: the achondroplasia family of skeletal dysplasias, Muenke craniosynostosis, and Crouzon syndrome with acanthosis nigricans. Endocr Rev. 2000 Feb;21(1):23-39. doi: 10.1210/edrv.21.1.0387. Citation on PubMed
- Wright MJ, Irving MD. Clinical management of achondroplasia. Arch Dis Child. 2012 Feb;97(2):129-34. doi: 10.1136/adc.2010.189092. Epub 2011 Apr 3. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.