

Description
Thiamine-responsive megaloblastic anemia syndrome (TRMA) is a rare condition that is characterized by hearing loss, diabetes, and a blood disorder called megaloblastic anemia. Megaloblastic anemia occurs when a person has a low number of red blood cells (anemia), and the red blood cells that are present are larger than normal (megaloblastic). The symptoms of this blood disorder may include decreased appetite, lack of energy, headaches, pale skin, diarrhea, and tingling or numbness in the hands and feet. Individuals with TRMA typically develop megaloblastic anemia between infancy and adolescence. TRMA is called "thiamine-responsive" because the anemia can be treated with daily doses of vitamin B1 (thiamine).
In people with TRMA, hearing loss typically develops during early childhood and is caused by abnormalities of the inner ear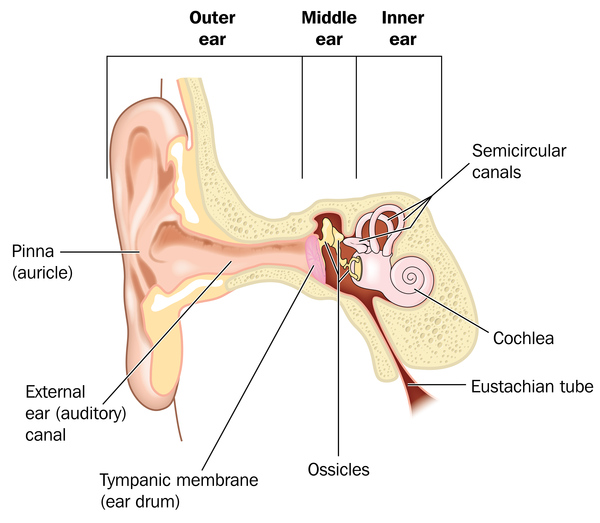 (sensorineural hearing loss). The hearing loss usually worsens over time. It remains unclear whether treatment with thiamine can improve hearing or delay hearing loss in people with TRMA.
(sensorineural hearing loss). The hearing loss usually worsens over time. It remains unclear whether treatment with thiamine can improve hearing or delay hearing loss in people with TRMA.
People with TRMA often develop diabetes mellitus, a condition in which glucose levels can become dangerously high, at an early age. Although some individuals with TRMA develop diabetes during childhood, they do not have the autoimmune form of diabetes that typically develops in children, called type 1 diabetes. People with TRMA usually require insulin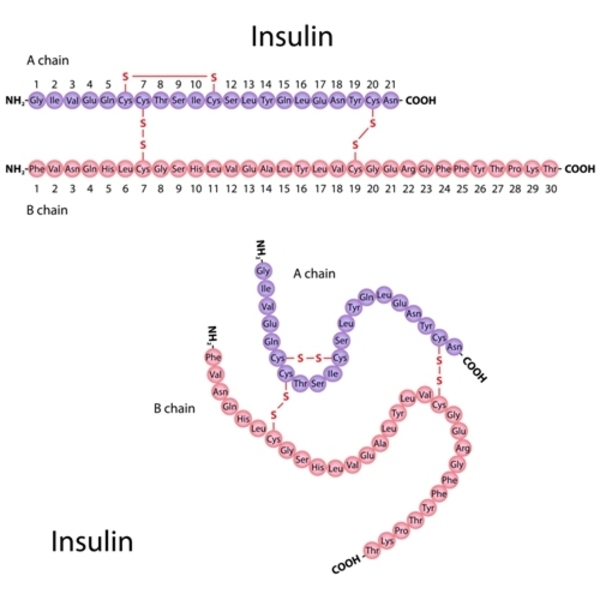 to treat their diabetes
to treat their diabetes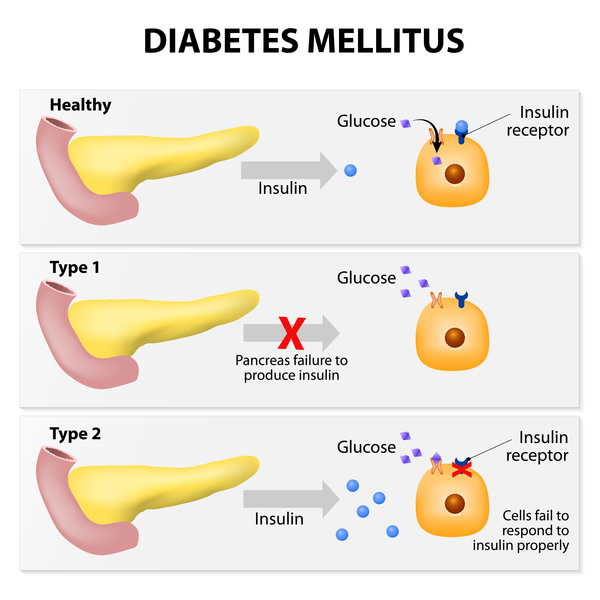 . In some cases, treatment with thiamine may delay the onset of diabetes or reduce the amount of insulin a person needs.
. In some cases, treatment with thiamine may delay the onset of diabetes or reduce the amount of insulin a person needs.
Some individuals with TRMA have abnormalities of the eye, including optic atrophy, which is the degeneration (atrophy) of the nerves that carry information from the eyes to the brain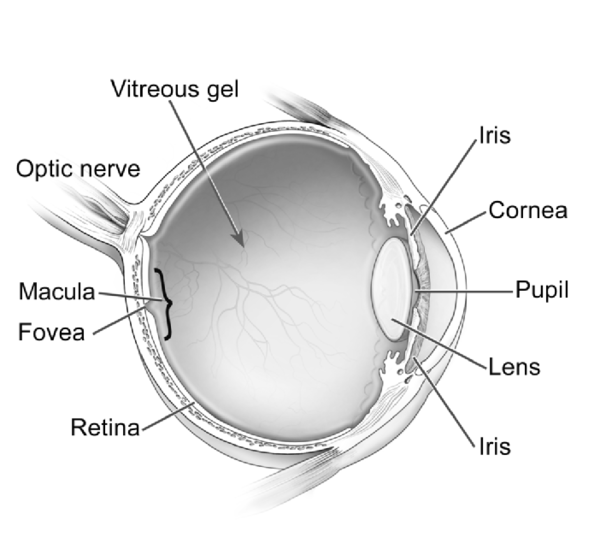 . Additional features of this condition may include heart and blood vessel (cardiovascular) problems, intellectual disabilities, behavioral changes, and seizures.
. Additional features of this condition may include heart and blood vessel (cardiovascular) problems, intellectual disabilities, behavioral changes, and seizures.
Frequency
TRMA is rare, though its exact prevalence is unknown. Approximately 200 individuals with this condition have been described in the medical literature.
Causes
Variants (also called mutations) in the SLC19A2 gene cause TRMA. This gene provides instructions for making a protein called thiamine transporter 1, which transports thiamine into cells. Thiamine is found in many different foods and is important for numerous body functions.
Most variants in the SLC19A2 gene lead to the production of an abnormally short, nonfunctional version of thiamine transporter 1. Other variants change single protein building blocks (amino acids ) in thiamine transporter 1. All of these variants disrupt the protein's ability to bring thiamine into the cell. TRMA is treated with daily doses of thiamine because some thiamine can pass into the cell without the help of a transporter when the vitamin is present in large amounts.
) in thiamine transporter 1. All of these variants disrupt the protein's ability to bring thiamine into the cell. TRMA is treated with daily doses of thiamine because some thiamine can pass into the cell without the help of a transporter when the vitamin is present in large amounts.
It remains unclear exactly how variants in the SLC19A2 gene cause the specific set of features seen in people with TRMA. Research suggests that an alternative transporter made by a different gene is available to transport thiamine in many tissues of the body. However, this alternative transporter may not be as active in the inner ear, the bone marrow (where blood cells are made), and the pancreas (where insulin is made), which would explain why these tissues are affected in people with TRMA.
Inheritance
This condition is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- Rogers syndrome
- Thiamine-responsive megaloblastic anemia with diabetes mellitus and sensorineural hearing loss
- TRMA
Additional Information & Resources
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Baron D, Assaraf YG, Cohen N, Aronheim A. Lack of plasma membrane targeting of a G172D mutant thiamine transporter derived from Rogers syndrome family. Mol Med. 2002 Aug;8(8):462-74. Citation on PubMed or Free article on PubMed Central
- Diaz GA, Banikazemi M, Oishi K, Desnick RJ, Gelb BD. Mutations in a new gene encoding a thiamine transporter cause thiamine-responsive megaloblastic anaemia syndrome. Nat Genet. 1999 Jul;22(3):309-12. doi: 10.1038/10385. Citation on PubMed
- Habeb AM, Flanagan SE, Zulali MA, Abdullah MA, Pomahacova R, Boyadzhiev V, Colindres LE, Godoy GV, Vasanthi T, Al Saif R, Setoodeh A, Haghighi A, Haghighi A, Shaalan Y; International Neonatal Diabetes Consortium; Hattersley AT, Ellard S, De Franco E. Pharmacogenomics in diabetes: outcomes of thiamine therapy in TRMA syndrome. Diabetologia. 2018 May;61(5):1027-1036. doi: 10.1007/s00125-018-4554-x. Epub 2018 Feb 15. Citation on PubMed
- Liberman MC, Tartaglini E, Fleming JC, Neufeld EJ. Deletion of SLC19A2, the high affinity thiamine transporter, causes selective inner hair cell loss and an auditory neuropathy phenotype. J Assoc Res Otolaryngol. 2006 Sep;7(3):211-7. doi: 10.1007/s10162-006-0035-x. Epub 2006 Apr 27. Citation on PubMed or Free article on PubMed Central
- Lorber A, Gazit AZ, Khoury A, Schwartz Y, Mandel H. Cardiac manifestations in thiamine-responsive megaloblastic anemia syndrome. Pediatr Cardiol. 2003 Sep-Oct;24(5):476-81. doi: 10.1007/s00246-002-0215-3. Citation on PubMed
- Olsen BS, Hahnemann JM, Schwartz M, Ostergaard E. Thiamine-responsive megaloblastic anaemia: a cause of syndromic diabetes in childhood. Pediatr Diabetes. 2007 Aug;8(4):239-41. doi: 10.1111/j.1399-5448.2007.00251.x. Citation on PubMed
- Ricketts CJ, Minton JA, Samuel J, Ariyawansa I, Wales JK, Lo IF, Barrett TG. Thiamine-responsive megaloblastic anaemia syndrome: long-term follow-up and mutation analysis of seven families. Acta Paediatr. 2006 Jan;95(1):99-104. doi: 10.1080/08035250500323715. Citation on PubMed
- Sako S, Tsunogai T, Oishi K. Thiamine-Responsive Megaloblastic Anemia Syndrome. 2003 Oct 24 [updated 2022 Jul 28]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1282/ Citation on PubMed
- Zhang S, Qiao Y, Wang Z, Zhuang J, Sun Y, Shang X, Li G. Identification of novel compound heterozygous variants in SLC19A2 and the genotype-phenotype associations in thiamine-responsive megaloblastic anemia. Clin Chim Acta. 2021 May;516:157-168. doi: 10.1016/j.cca.2021.01.025. Epub 2021 Feb 9. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.