

Description
Polycystic lipomembranous osteodysplasia with sclerosing leukoencephalopathy, commonly known as PLOSL, is a progressive disorder that affects the bones and brain. "Polycystic lipomembranous osteodysplasia" refers to cyst-like bone changes that can be seen on x-rays. "Sclerosing leukoencephalopathy" describes specific changes in the brain that are found in people with this disorder.
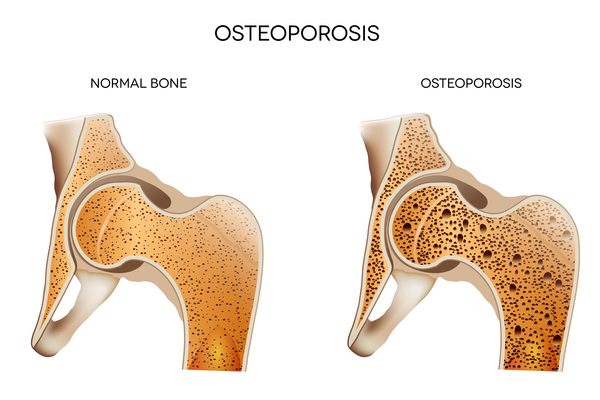
The bone abnormalities associated with PLOSL usually become apparent in a person's twenties. In most affected individuals, pain and tenderness in the ankles and feet are the first symptoms of the disease. Several years later, broken bones (fractures) begin to occur frequently, particularly in the bones of the ankles, feet, wrists, and hands. Bone pain and fractures are caused by thinning of the bones (osteoporosis) and cysts in the bones. These abnormalities weaken bones and make them more likely to break.
The brain abnormalities characteristic of PLOSL typically appear in a person's thirties. Personality changes are among the first noticeable problems, followed by a loss of judgment, feelings of intense happiness (euphoria), a loss of inhibition, and poor concentration. These neurologic changes cause significant problems in an affected person's social and family life. As the disease progresses, it causes a severe decline in thinking and reasoning abilities (dementia). Affected people ultimately become unable to walk, speak, or care for themselves. People with this disease usually live only into their thirties or forties.
Frequency
PLOSL is a very rare condition. It was first reported in the Finnish population, where it has an estimated prevalence of 1 to 2 per million people. This condition has also been diagnosed in more than 100 people in the Japanese population. Although affected individuals have been reported worldwide, PLOSL appears to be less common in other countries.
Causes
Variants (also called mutations) in the TREM2 gene or the TYROBP gene can cause PLOSL. The proteins produced from these two genes work together to activate certain kinds of cells. These proteins appear to be particularly important in osteoclasts, which are specialized cells that break down and remove (resorb) bone tissue that is no longer needed. Osteoclasts are involved in bone remodeling, which is a normal process that replaces old bone tissue with new bone. The TREM2 and TYROBP proteins are also critical for the normal function of microglia, which are a type of immune cell in the brain and spinal cord (central nervous system). Although these proteins play essential roles in osteoclasts and microglia, their exact function in these cells is unclear.
Variants in the TREM2 or TYROBP gene disrupt normal bone remodeling and lead to progressive brain abnormalities in people with PLOSL. Researchers believe that the bone changes seen in people with this disorder are related to malfunctioning osteoclasts, which are less able to resorb bone tissue during bone remodeling. In the central nervous system, TREM2 or TYROBP gene variants cause widespread abnormalities of microglia. Researchers are working to determine how these abnormalities lead to the neurological problems associated with PLOSL.
Inheritance
This condition is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- Nasu-Hakola disease
- NHD
- PLO-SL
- PLOSL
- Presenile dementia with bone cysts
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Klunemann HH, Ridha BH, Magy L, Wherrett JR, Hemelsoet DM, Keen RW, De Bleecker JL, Rossor MN, Marienhagen J, Klein HE, Peltonen L, Paloneva J. The genetic causes of basal ganglia calcification, dementia, and bone cysts: DAP12 and TREM2. Neurology. 2005 May 10;64(9):1502-7. doi: 10.1212/01.WNL.0000160304.00003.CA. Citation on PubMed
- Kondo T, Takahashi K, Kohara N, Takahashi Y, Hayashi S, Takahashi H, Matsuo H, Yamazaki M, Inoue K, Miyamoto K, Yamamura T. Heterogeneity of presenile dementia with bone cysts (Nasu-Hakola disease): three genetic forms. Neurology. 2002 Oct 8;59(7):1105-7. doi: 10.1212/wnl.59.7.1105. Citation on PubMed
- Madry H, Prudlo J, Grgic A, Freyschmidt J. Nasu-Hakola disease (PLOSL): report of five cases and review of the literature. Clin Orthop Relat Res. 2007 Jan;454:262-9. doi: 10.1097/01.blo.0000229364.57985.df. Citation on PubMed
- Paloneva J, Autti T, Raininko R, Partanen J, Salonen O, Puranen M, Hakola P, Haltia M. CNS manifestations of Nasu-Hakola disease: a frontal dementia with bone cysts. Neurology. 2001 Jun 12;56(11):1552-8. doi: 10.1212/wnl.56.11.1552. Citation on PubMed
- Paloneva J, Autti T, Solje E, Haltia MJ. Polycystic Lipomembranous Osteodysplasia with Sclerosing Leukoencephalopathy. 2002 Jan 24 [updated 2026 Apr 7]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1197/ Citation on PubMed
- Verloes A, Maquet P, Sadzot B, Vivario M, Thiry A, Franck G. Nasu-Hakola syndrome: polycystic lipomembranous osteodysplasia with sclerosing leucoencephalopathy and presenile dementia. J Med Genet. 1997 Sep;34(9):753-7. doi: 10.1136/jmg.34.9.753. No abstract available. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.