

Description
Lysosomal acid lipase deficiency is an inherited condition characterized by problems with the breakdown and use of fats and cholesterol in the body (lipid metabolism). In affected individuals, harmful amounts of fats (lipids) accumulate in cells and tissues throughout the body, which typically causes liver disease. There are two forms of the condition. The most severe and rarest form begins in infancy. The less severe form can begin from childhood to late adulthood.
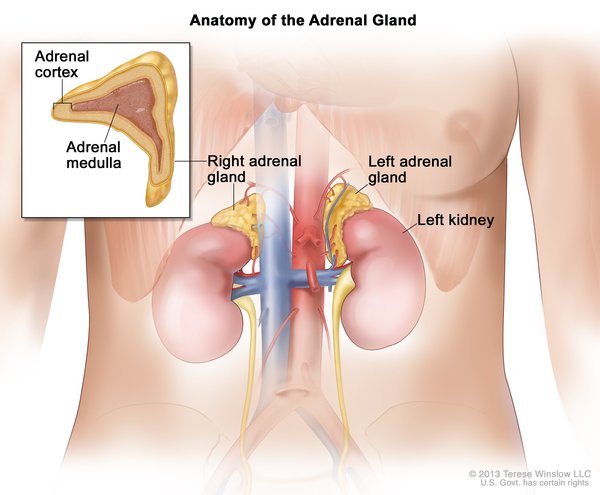
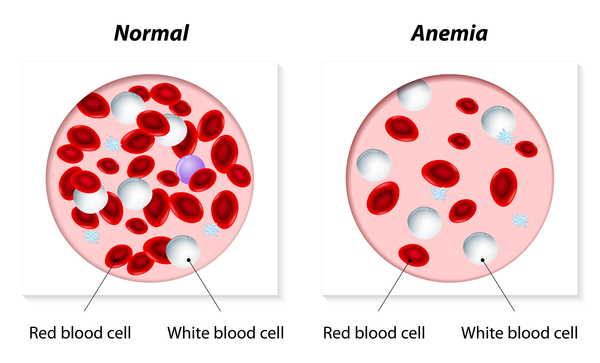
In the severe, early-onset form of lysosomal acid lipase deficiency, lipids accumulate throughout the body, particularly in the liver, within the first weeks of life. This accumulation of lipids leads to several health problems, including an enlarged liver and spleen (hepatosplenomegaly), poor weight gain, a yellow tint to the skin and the whites of the eyes (jaundice), vomiting, diarrhea, fatty stool (steatorrhea), and poor absorption of nutrients from food (malabsorption). In addition, affected infants often have calcium deposits in small hormone-producing glands on top of each kidney (adrenal glands), low amounts of iron in the blood (anemia), and developmental delay. Scar tissue quickly builds up in the liver, leading to liver disease (cirrhosis). Infants with this form of lysosomal acid lipase deficiency develop multi-organ failure and severe malnutrition and generally do not survive past 1 year.
In the later-onset form of lysosomal acid lipase deficiency, signs and symptoms vary and usually begin in mid-childhood, although they can appear anytime up to late adulthood. Nearly all affected individuals develop an enlarged liver (hepatomegaly); an enlarged spleen (splenomegaly) may also occur. About two-thirds of individuals have liver fibrosis, eventually leading to cirrhosis. Approximately one-third of individuals with the later-onset form have malabsorption, diarrhea, vomiting, and steatorrhea. Individuals with this form of lysosomal acid lipase deficiency may have increased liver enzymes and high cholesterol levels, which can be detected with blood tests.
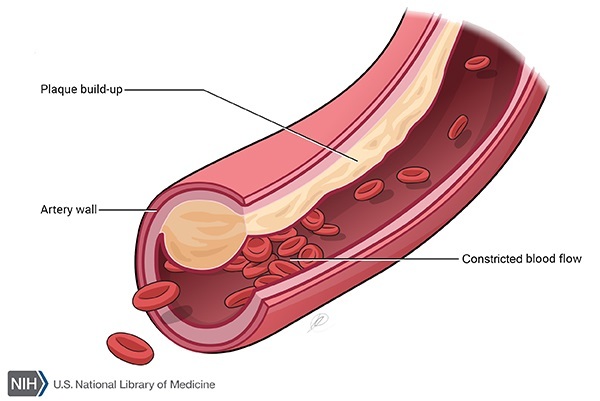
Some people with this later-onset form of lysosomal acid lipase deficiency develop an accumulation of fatty deposits on the artery walls (atherosclerosis). Although these deposits are common in the general population, they usually begin at an earlier age in people with lysosomal acid lipase deficiency. The deposits narrow the arteries, increasing the chance of heart attack or stroke. The expected lifespan of individuals with later-onset lysosomal acid lipase deficiency depends on the severity of the associated health problems.
The two forms of lysosomal acid lipase deficiency were once thought to be separate disorders. The early-onset form was known as Wolman disease, and the later-onset form was known as cholesteryl ester storage disease. Although these two disorders have the same genetic cause and are now considered to be forms of a single condition, these names are still sometimes used to distinguish between the forms of lysosomal acid lipase deficiency.
Frequency
Lysosomal acid lipase deficiency is estimated to occur in 1 in 40,000 to 300,000 individuals, varying by population. The later-onset form is more common than the early-onset form.
Causes
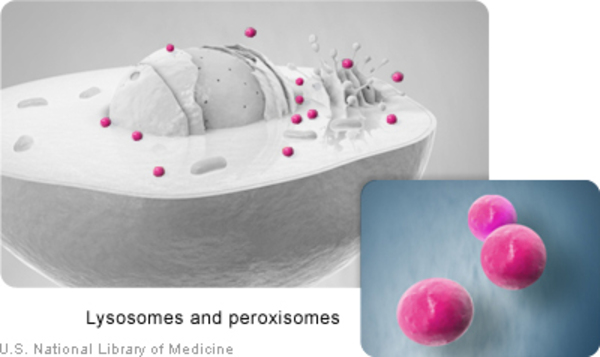
Mutations in the LIPA gene cause lysosomal acid lipase deficiency. The LIPA gene provides instructions for producing an enzyme called lysosomal acid lipase. This enzyme is found in cell compartments called lysosomes, which digest and recycle materials the cell no longer needs. The lysosomal acid lipase enzyme breaks down lipids such as cholesteryl esters and triglycerides. The lipids produced through these processes, cholesterol and fatty acids, are used by the body or transported to the liver for removal.
Mutations in the LIPA gene lead to a shortage (deficiency) of functional lysosomal acid lipase. The severity of the condition depends on how much working enzyme is available. Individuals with the early-onset form of lysosomal acid lipase deficiency have no normal enzyme activity. Those with the later-onset form are thought to have some enzyme activity remaining, and the amount generally determines the severity of signs and symptoms.
Decreased lysosomal acid lipase activity results in the accumulation of cholesteryl esters, triglycerides, and other lipids within lysosomes, causing fat buildup in multiple tissues. The body's inability to produce cholesterol from the breakdown of these lipids leads to an increase in alternative methods of cholesterol production and higher-than-normal levels of cholesterol in the blood. The excess lipids are transported to the liver for removal. Because many of them are not broken down properly, they cannot be removed from the body; instead they accumulate in the liver, resulting in liver disease. The progressive accumulation of lipids in tissues results in organ dysfunction and the signs and symptoms of lysosomal acid lipase deficiency.
Inheritance
This condition is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.

Other Names for This Condition
- Acid esterase deficiency
- Acid lipase deficiency
- Familial visceral xanthomatosis
- Familial xanthomatosis
- LAL deficiency
- LIPA deficiency
- Primary familial xanthomatosis
- Primary familial xanthomatosis with adrenal calcification
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Burton BK, Deegan PB, Enns GM, Guardamagna O, Horslen S, Hovingh GK, Lobritto SJ, Malinova V, McLin VA, Raiman J, Di Rocco M, Santra S, Sharma R, Sykut-Cegielska J, Whitley CB, Eckert S, Valayannopoulos V, Quinn AG. Clinical Features of Lysosomal Acid Lipase Deficiency. J Pediatr Gastroenterol Nutr. 2015 Dec;61(6):619-25. doi: 10.1097/MPG.0000000000000935. Citation on PubMed or Free article on PubMed Central
- Reiner Z, Guardamagna O, Nair D, Soran H, Hovingh K, Bertolini S, Jones S, Coric M, Calandra S, Hamilton J, Eagleton T, Ros E. Lysosomal acid lipase deficiency--an under-recognized cause of dyslipidaemia and liver dysfunction. Atherosclerosis. 2014 Jul;235(1):21-30. doi: 10.1016/j.atherosclerosis.2014.04.003. Epub 2014 Apr 15. Citation on PubMed
- Saito S, Ohno K, Suzuki T, Sakuraba H. Structural bases of Wolman disease and cholesteryl ester storage disease. Mol Genet Metab. 2012 Feb;105(2):244-8. doi: 10.1016/j.ymgme.2011.11.004. Epub 2011 Nov 20. Citation on PubMed
- Zhang B, Porto AF. Cholesteryl ester storage disease: protean presentations of lysosomal acid lipase deficiency. J Pediatr Gastroenterol Nutr. 2013 Jun;56(6):682-5. doi: 10.1097/MPG.0b013e31828b36ac. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.