

Description
Kleefstra syndrome is a disorder that involves many parts of the body. Characteristic features of Kleefstra syndrome include developmental delay and intellectual disability, severely limited or absent speech, and weak muscle tone (hypotonia). Affected individuals also have an unusually small head size (microcephaly) and a wide, short skull (brachycephaly). Distinctive facial features include eyebrows that grow together in the middle (synophrys), widely spaced eyes (hypertelorism), a sunken appearance of the middle of the face (midface hypoplasia), nostrils that open to the front rather than downward (anteverted nares), a protruding jaw (prognathism), rolled out (everted) lips, and a large tongue (macroglossia). Affected individuals may have a high birth weight and childhood obesity.




People with Kleefstra syndrome may also have structural brain abnormalities, congenital heart defects, genitourinary abnormalities, seizures, and a tendency to develop severe respiratory infections. During childhood they may exhibit features of autism or related developmental disorders affecting communication and social interaction. In adolescence, they may develop a general loss of interest and enthusiasm (apathy) or unresponsiveness (catatonia).
Frequency
The prevalence of Kleefstra syndrome is unknown. Only recently has testing become available to distinguish it from other disorders with similar features.
Causes
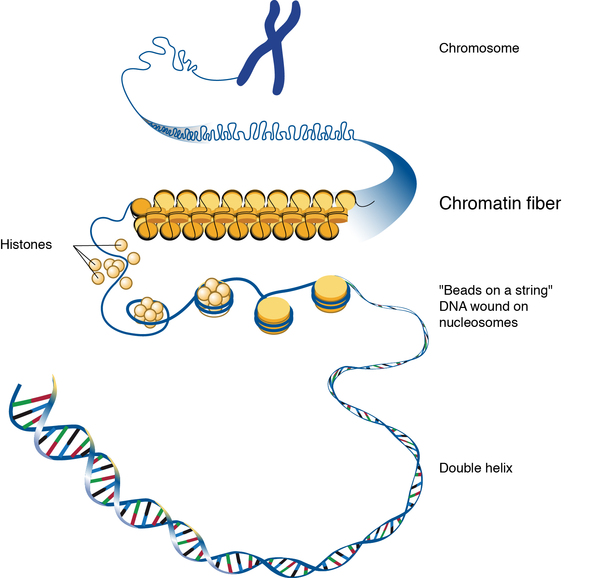
Kleefstra syndrome is caused by the loss of the EHMT1 gene or by mutations that disable its function. The EHMT1 gene provides instructions for making an enzyme called euchromatic histone methyltransferase 1. Histone methyltransferases are enzymes that modify proteins called histones. Histones are structural proteins that attach (bind) to DNA and give chromosomes their shape. By adding a molecule called a methyl group to histones, histone methyltransferases can turn off (suppress) the activity of certain genes, which is essential for normal development and function.
Most people with Kleefstra syndrome are missing a sequence of about 1 million DNA building blocks (base pairs) on one copy of chromosome 9 in each cell. The deletion occurs near the end of the long (q) arm of the chromosome at a location designated q34.3, a region containing the EHMT1 gene. Some affected individuals have shorter or longer deletions in the same region.
The loss of the EHMT1 gene from one copy of chromosome 9 in each cell is believed to be responsible for the characteristic features of Kleefstra syndrome in people with the 9q34.3 deletion. However, the loss of other genes in the same region may lead to additional health problems in some affected individuals.
About 25 percent of individuals with Kleefstra syndrome do not have a deletion of genetic material from chromosome 9; instead, these individuals have mutations in the EHMT1 gene. Some of these mutations change single protein building blocks (amino acids) in euchromatic histone methyltransferase 1. Others create a premature stop signal in the instructions for making the enzyme or alter the way the gene's instructions are pieced together to produce the enzyme. These changes generally result in an enzyme that is unstable and decays rapidly, or that is disabled and cannot function properly.
Either a deletion or a mutation affecting the EHMT1 gene results in a lack of functional euchromatic histone methyltransferase 1 enzyme. A lack of this enzyme impairs proper control of the activity of certain genes in many of the body's organs and tissues, resulting in the abnormalities of development and function characteristic of Kleefstra syndrome.
Inheritance
The inheritance of Kleefstra syndrome is considered to be autosomal dominant because a deletion in one copy of chromosome 9 in each cell or a mutation in one copy of the EHMT1 gene is sufficient to cause the condition. Most cases of Kleefstra syndrome are not inherited, however. The genetic change occurs most often as a random event during the formation of reproductive cells (eggs or sperm) or in early fetal development. Affected people typically have no history of the disorder in their family, though they can pass the disorder on to their children. Only a few people with Kleefstra syndrome have been known to reproduce.


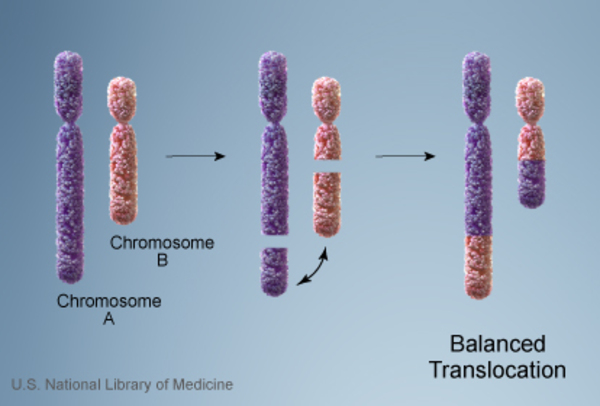
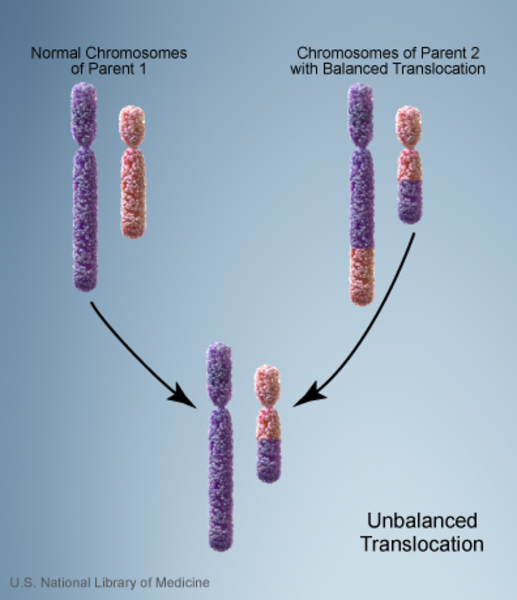
Rarely, affected individuals inherit a chromosome 9 with a deleted segment from an unaffected parent. In these cases, the parent carries a chromosomal rearrangement called a balanced translocation, in which no genetic material is gained or lost. Balanced translocations usually do not cause any health problems; however, they can become unbalanced as they are passed to the next generation. Children who inherit an unbalanced translocation can have a chromosomal rearrangement with extra or missing genetic material. Individuals with Kleefstra syndrome who inherit an unbalanced translocation are missing genetic material from the long arm of chromosome 9.
A few individuals with Kleefstra syndrome have inherited the chromosome 9q34.3 deletion from an unaffected parent who is mosaic for the deletion. Mosaic means that an individual has the deletion in some cells (including some sperm or egg cells), but not in others.
Other Names for This Condition
- 9q subtelomeric deletion syndrome
- 9q- syndrome
- 9q34.3 deletion syndrome
- 9q34.3 microdeletion syndrome
- Chromosome 9q deletion syndrome
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Iwakoshi M, Okamoto N, Harada N, Nakamura T, Yamamori S, Fujita H, Niikawa N, Matsumoto N. 9q34.3 deletion syndrome in three unrelated children. Am J Med Genet A. 2004 Apr 30;126A(3):278-83. doi: 10.1002/ajmg.a.20602. Citation on PubMed
- Kleefstra T, Brunner HG, Amiel J, Oudakker AR, Nillesen WM, Magee A, Genevieve D, Cormier-Daire V, van Esch H, Fryns JP, Hamel BC, Sistermans EA, de Vries BB, van Bokhoven H. Loss-of-function mutations in euchromatin histone methyl transferase 1 (EHMT1) cause the 9q34 subtelomeric deletion syndrome. Am J Hum Genet. 2006 Aug;79(2):370-7. doi: 10.1086/505693. Epub 2006 Jun 13. Citation on PubMed or Free article on PubMed Central
- Kleefstra T, de Leeuw N. Kleefstra Syndrome. 2010 Oct 5 [updated 2023 Jan 26]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK47079/ Citation on PubMed
- Kleefstra T, Smidt M, Banning MJ, Oudakker AR, Van Esch H, de Brouwer AP, Nillesen W, Sistermans EA, Hamel BC, de Bruijn D, Fryns JP, Yntema HG, Brunner HG, de Vries BB, van Bokhoven H. Disruption of the gene Euchromatin Histone Methyl Transferase1 (Eu-HMTase1) is associated with the 9q34 subtelomeric deletion syndrome. J Med Genet. 2005 Apr;42(4):299-306. doi: 10.1136/jmg.2004.028464. Citation on PubMed or Free article on PubMed Central
- Kleefstra T, van Zelst-Stams WA, Nillesen WM, Cormier-Daire V, Houge G, Foulds N, van Dooren M, Willemsen MH, Pfundt R, Turner A, Wilson M, McGaughran J, Rauch A, Zenker M, Adam MP, Innes M, Davies C, Lopez AG, Casalone R, Weber A, Brueton LA, Navarro AD, Bralo MP, Venselaar H, Stegmann SP, Yntema HG, van Bokhoven H, Brunner HG. Further clinical and molecular delineation of the 9q subtelomeric deletion syndrome supports a major contribution of EHMT1 haploinsufficiency to the core phenotype. J Med Genet. 2009 Sep;46(9):598-606. doi: 10.1136/jmg.2008.062950. Epub 2009 Mar 4. Citation on PubMed
- Neas KR, Smith JM, Chia N, Huseyin S, St Heaps L, Peters G, Sholler G, Tzioumi D, Sillence DO, Mowat D. Three patients with terminal deletions within the subtelomeric region of chromosome 9q. Am J Med Genet A. 2005 Feb 1;132A(4):425-30. doi: 10.1002/ajmg.a.30496. Citation on PubMed
- Stewart DR, Kleefstra T. The chromosome 9q subtelomere deletion syndrome. Am J Med Genet C Semin Med Genet. 2007 Nov 15;145C(4):383-92. doi: 10.1002/ajmg.c.30148. Citation on PubMed
- Verhoeven WM, Egger JI, Vermeulen K, van de Warrenburg BP, Kleefstra T. Kleefstra syndrome in three adult patients: further delineation of the behavioral and neurological phenotype shows aspects of a neurodegenerative course. Am J Med Genet A. 2011 Oct;155A(10):2409-15. doi: 10.1002/ajmg.a.34186. Epub 2011 Sep 9. Citation on PubMed
- Willemsen MH, Beunders G, Callaghan M, de Leeuw N, Nillesen WM, Yntema HG, van Hagen JM, Nieuwint AW, Morrison N, Keijzers-Vloet ST, Hoischen A, Brunner HG, Tolmie J, Kleefstra T. Familial Kleefstra syndrome due to maternal somatic mosaicism for interstitial 9q34.3 microdeletions. Clin Genet. 2011 Jul;80(1):31-8. doi: 10.1111/j.1399-0004.2010.01607.x. Epub 2011 Jan 10. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.