

Description
Huntington's disease-like (HDL) is a group of related neurological conditions. As the name suggests, HDLs resembles Huntington's disease. HDLs and Huntington's disease are both characterized by uncontrolled movements, emotional problems, and loss of thinking ability. In both conditions these signs and symptoms worsen over time. HDLs occurs in people with the characteristic features of Huntington's disease who do not have a variant (also called mutation) in the gene typically associated with that disorder. Researchers have described four HDLs that are designated Huntington's disease-like 1 (HDL1) through Huntington's disease-like 4 (HDL4). Sometimes, HDL4 is also known as spinocerebellar ataxia type 17 (SCA17).
HDL1, HDL2, and HDL4 usually begin in early to mid-adulthood, although they can start earlier or later. The first signs and symptoms of these conditions often include irritability, emotional problems, small involuntary movements (dyskinesia), poor coordination, and trouble learning new information or making decisions. Many people with an HDL develop involuntary jerking or twitching movements known as chorea. Over time, these abnormal movements worsen. Affected individuals may develop problems with walking (bradykinesia), speaking (dysarthria), and swallowing (dysphagia). People with these disorders also experience changes in personality and a decline in thinking and reasoning abilities (dementia). Individuals with an HDL syndrome can live for 10 to 20 years after signs and symptoms begin, though this can vary between the types of HDL syndromes.
HDL3 begins much earlier in life than the other HDLs (usually around age 3 or 4). Affected children experience a decline in thinking ability, difficulties with movement and speech, and seizures. Because HDL3 has some different signs and symptoms and a different pattern of inheritance, researchers are unsure whether it belongs in the same category as the other HDLs.
Frequency
Overall, HDLs are rare. They are much less common than Huntington's disease, which affects an estimated 3 to 7 per 100,000 people of European ancestry.
Of the four described HDLs, HDL4 appears to be the most common. HDL2 is the second most common and occurs almost exclusively in people of African ancestry (especially Black South Africans).
Causes
Variants in the PRNP, JPH3, and TBP genes have been found to cause the various HDLs. HDL1 is caused by variants in the PRNP gene, while HDL2 is caused by variants in JPH3. Variants in the TBP gene are responsible for HDL4. The genetic cause of HDL3 is unknown. These variants may account for some of the people with characteristic features of Huntington's disease who do not have a variant in the gene typically associated with that disorder.
The PRNP, JPH3, and TBP genes provide instructions for making proteins that are important for normal brain function. The features of HDLs result from a particular type of variant in any one of these genes. Normally, these genes contain a segment of DNA that repeats multiple times in a row. The variants that cause HDLs increase the length of these repeated segments. This type of variant leads to the production of an abnormal PRNP, JPH3, or TBP protein. As a result, there is a loss in normal protein activity. Additionally, the abnormal protein can build up in nerve cells (neurons) and disrupt the normal functions of these cells. The dysfunction and eventual death of neurons in certain areas of the brain underlie the signs and symptoms of each HDL.
Many other medical conditions may also cause signs and symptoms that resemble those seen in people with Huntington's disease. This can make it difficult to accurately diagnose these conditions.
Inheritance
HDL1, HDL2, and HDL4 are inherited in an autosomal dominant pattern , which means one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases of HDLs, an affected person has one parent with the condition.
, which means one copy of the altered gene in each cell is sufficient to cause the disorder. In most cases of HDLs, an affected person has one parent with the condition.
HDL2 and HDL4 generally begin earlier in life and have more severe symptoms as the variants that cause these disorders are passed down from one generation to the next. This phenomenon is known as anticipation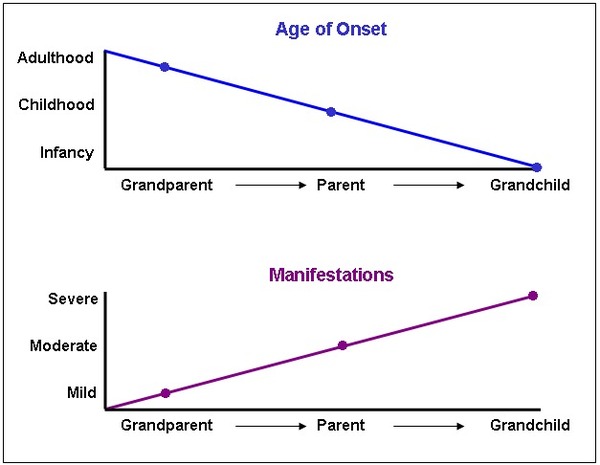 . Anticipation is caused by an increase in the length of an unstable region in the gene.
. Anticipation is caused by an increase in the length of an unstable region in the gene.
HDL3 is probably inherited in an autosomal recessive pattern , which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- HDL
- HDL syndrome
- Huntington disease-like syndrome
- Huntington disease-like syndromes
- Huntington's disease phenocopies
- Huntington's disease phenocopy syndromes
- Huntington's disease-like syndrome
- Huntington's disease-like syndromes
Additional Information & Resources
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Anderson DG, Krause A, Margolis RL. Huntington Disease-Like 2. 2004 Jan 30 [updated 2025 Apr 10]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1529/ Citation on PubMed
- Dupre N, Rouleau G. The Puzzle of Huntington Disease Phenocopies. JAMA Neurol. 2016 Sep 1;73(9):1056-8. doi: 10.1001/jamaneurol.2016.2095. No abstract available. Citation on PubMed
- Krause A, Mitchell C, Essop F, Tager S, Temlett J, Stevanin G, Ross C, Rudnicki D, Margolis R. Junctophilin 3 (JPH3) expansion mutations causing Huntington disease like 2 (HDL2) are common in South African patients with African ancestry and a Huntington disease phenotype. Am J Med Genet B Neuropsychiatr Genet. 2015 Oct;168(7):573-85. doi: 10.1002/ajmg.b.32332. Epub 2015 Jun 16. Citation on PubMed
- Mariani LL, Tesson C, Charles P, Cazeneuve C, Hahn V, Youssov K, Freeman L, Grabli D, Roze E, Noel S, Peuvion JN, Bachoud-Levi AC, Brice A, Stevanin G, Durr A. Expanding the Spectrum of Genes Involved in Huntington Disease Using a Combined Clinical and Genetic Approach. JAMA Neurol. 2016 Sep 1;73(9):1105-14. doi: 10.1001/jamaneurol.2016.2215. Citation on PubMed
- Schneider SA, Bird T. Huntington's Disease, Huntington's Disease Look-Alikes, and Benign Hereditary Chorea: What's New? Mov Disord Clin Pract. 2016 Jan 27;3(4):342-354. doi: 10.1002/mdc3.12312. eCollection 2016 Jul-Aug. Citation on PubMed
- Schneider SA, Walker RH, Bhatia KP. The Huntington's disease-like syndromes: what to consider in patients with a negative Huntington's disease gene test. Nat Clin Pract Neurol. 2007 Sep;3(9):517-25. doi: 10.1038/ncpneuro0606. Citation on PubMed
- Stevanin G, Fujigasaki H, Lebre AS, Camuzat A, Jeannequin C, Dode C, Takahashi J, San C, Bellance R, Brice A, Durr A. Huntington's disease-like phenotype due to trinucleotide repeat expansions in the TBP and JPH3 genes. Brain. 2003 Jul;126(Pt 7):1599-603. doi: 10.1093/brain/awg155. Epub 2003 May 6. Citation on PubMed
- Toyoshima Y, Onodera O, Yamada M, Tsuji S, Takahashi H. Spinocerebellar Ataxia Type 17. 2005 Mar 29 [updated 2022 Jul 28]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1438/ Citation on PubMed
- Wild EJ, Mudanohwo EE, Sweeney MG, Schneider SA, Beck J, Bhatia KP, Rossor MN, Davis MB, Tabrizi SJ. Huntington's disease phenocopies are clinically and genetically heterogeneous. Mov Disord. 2008 Apr 15;23(5):716-20. doi: 10.1002/mds.21915. Citation on PubMed
- Wild EJ, Tabrizi SJ. Huntington's disease phenocopy syndromes. Curr Opin Neurol. 2007 Dec;20(6):681-7. doi: 10.1097/WCO.0b013e3282f12074. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.