

Description
GM2 activator deficiency (sometimes called GM2 gangliosidosis, AB variant) is a rare inherited disorder that causes progressive brain injury.
Most individuals with GM2 activator deficiency have the acute infantile form of the disease. Signs and symptoms of acute infantile GM2 activator deficiency typically appear between the ages of 4 and 12 months, when development slows and the muscles used for movement weaken. Infants with acute infantile GM2 activator deficiency stop achieving normal developmental milestones and eventually lose previously acquired skills such as turning over, sitting, and crawling. These infants also develop an exaggerated startle reaction to loud noises. Over time, infants with acute infantile GM2 activator deficiency typically experience seizures, vision loss, and intellectual disabilites. They eventually become unable to respond to their environment. An eye abnormality called a cherry-red spot, which can be identified with an eye examination, is characteristic of the infantile form of this disorder. Infants with acute infantile GM2 activator deficiency may survive into early childhood.
Some people with GM2 activator deficiency may develop milder and more variable signs and symptoms later in life. Due to the rarity of this condition, the full spectrum of the late-onset presentation has not been clearly defined.
Frequency
GM2 activator deficiency is extremely rare; fewer than 30 cases have been reported worldwide.
Causes
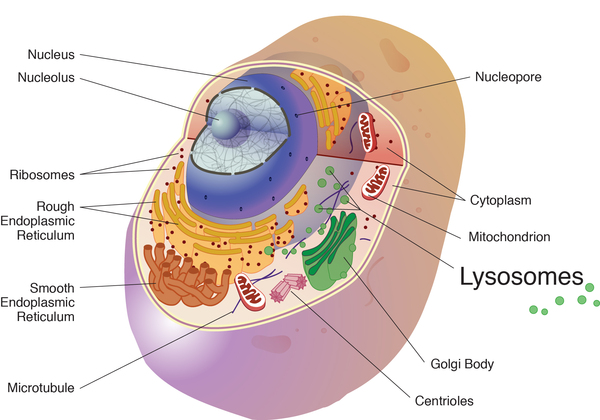
Variants (also called mutations) in the GM2A gene cause GM2 activator deficiency. The GM2A gene provides instructions for making a protein called the ganglioside GM2 activator. This protein is required for the normal function of an enzyme called beta-hexosaminidase A. Beta-hexosaminidase A and the ganglioside GM2 activator protein work together in lysosomes, which are compartments in the cell that digest and recycle different types of molecules. Within lysosomes, the activator protein binds to a fatty substance called GM2 ganglioside and presents it to beta-hexosaminidase A to be broken down.
Variants in the GM2A gene disrupt the activity of the ganglioside GM2 activator, which prevents beta-hexosaminidase A from breaking down GM2 ganglioside. As a result, this substance accumulates in the body, particularly in the central nervous system. Over time, damage caused by the buildup of GM2 ganglioside leads to the typical signs and symptoms of GM2 activator deficiency.
Because GM2 activator deficiency impairs the function of a lysosomal enzyme and involves the buildup of GM2 ganglioside, this condition is sometimes referred to as a lysosomal storage disorder or a GM2-gangliosidosis.
Inheritance
This condition is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell must have a variant to cause the disorder. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- GM2 gangliosidosis, AB variant
- Hexosaminidase activator deficiency
- Tay-Sachs disease, AB variant
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Chen B, Rigat B, Curry C, Mahuran DJ. Structure of the GM2A gene: identification of an exon 2 nonsense mutation and a naturally occurring transcript with an in-frame deletion of exon 2. Am J Hum Genet. 1999 Jul;65(1):77-87. doi: 10.1086/302463. Citation on PubMed or Free article on PubMed Central
- Ganne B, Dauriat B, Richard L, Lamari F, Ghorab K, Magy L, Benkirane M, Perani A, Marquet V, Calvas P, Yardin C, Bourthoumieu S. GM2 gangliosidosis AB variant: first case of late onset and review of the literature. Neurol Sci. 2022 Nov;43(11):6517-6527. doi: 10.1007/s10072-022-06270-x. Epub 2022 Aug 4. Citation on PubMed
- Mahuran DJ. Biochemical consequences of mutations causing the GM2 gangliosidoses. Biochim Biophys Acta. 1999 Oct 8;1455(2-3):105-38. doi: 10.1016/s0925-4439(99)00074-5. Citation on PubMed
- Martins C, Brunel-Guitton C, Lortie A, Gauvin F, Morales CR, Mitchell GA, Pshezhetsky AV. Atypical juvenile presentation of GM2 gangliosidosis AB in a patient compound-heterozygote for c.259G > T and c.164C > T mutations in the GM2A gene. Mol Genet Metab Rep. 2017 Apr 7;11:24-29. doi: 10.1016/j.ymgmr.2017.01.017. eCollection 2017 Jun. Citation on PubMed
- Sakuraba H, Itoh K, Shimmoto M, Utsumi K, Kase R, Hashimoto Y, Ozawa T, Ohwada Y, Imataka G, Eguchi M, Furukawa T, Schepers U, Sandhoff K. GM2 gangliosidosis AB variant: clinical and biochemical studies of a Japanese patient. Neurology. 1999 Jan 15;52(2):372-7. doi: 10.1212/wnl.52.2.372. Citation on PubMed
- Salih MA, Seidahmed MZ, El Khashab HY, Hamad MH, Bosley TM, Burn S, Myers A, Landsverk ML, Crotwell PL, Bilguvar K, Mane S, Kruer MC. Mutation in GM2A Leads to a Progressive Chorea-dementia Syndrome. Tremor Other Hyperkinet Mov (N Y). 2015 Jul 9;5:306. doi: 10.7916/D8D21WQ0. eCollection 2015. Citation on PubMed
- Schepers U, Glombitza G, Lemm T, Hoffmann A, Chabas A, Ozand P, Sandhoff K. Molecular analysis of a GM2-activator deficiency in two patients with GM2-gangliosidosis AB variant. Am J Hum Genet. 1996 Nov;59(5):1048-56. Citation on PubMed or Free article on PubMed Central
- Xiao C, Toro C, Tifft C. GM2 Activator Deficiency. 2022 Aug 25. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK583219/ Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.