

Description
GLUT1 deficiency syndrome is a disorder affecting the nervous system that can have a variety of neurological signs and symptoms. Approximately 90 percent of affected individuals have a form of the disorder often referred to as common GLUT1 deficiency syndrome. These individuals generally have frequent seizures (epilepsy) beginning in the first months of life. In newborns, the first sign of the disorder may be involuntary eye movements that are rapid and irregular. Babies with common GLUT1 deficiency syndrome have a normal head size at birth, but growth of the brain and skull is often slow, which can result in an abnormally small head size (microcephaly). People with this form of GLUT1 deficiency syndrome may have developmental delay or intellectual disability. Most affected individuals also have other neurological problems, such as stiffness caused by abnormal tensing of the muscles (spasticity), difficulty in coordinating movements (ataxia), and speech difficulties (dysarthria). Some experience episodes of confusion, lack of energy (lethargy), headaches, or muscle twitches (myoclonus), particularly during periods without food (fasting).
About 10 percent of individuals with GLUT1 deficiency syndrome have a form of the disorder often known as non-epileptic GLUT1 deficiency syndrome, which is usually less severe than the common form. People with the non-epileptic form do not have seizures, but they may still have developmental delay and intellectual disability. Most have movement problems such as ataxia or involuntary tensing of various muscles (dystonia); the movement problems may be more pronounced than in the common form.
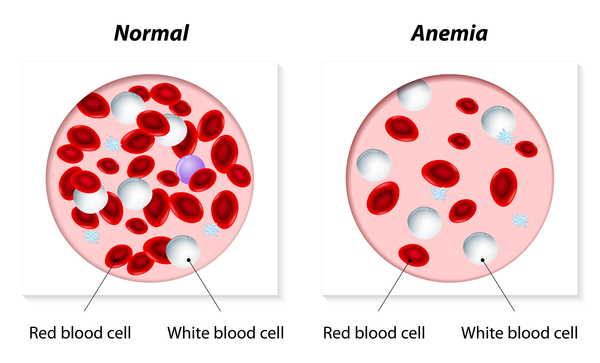
Several conditions that were originally given other names have since been recognized to be variants of GLUT1 deficiency syndrome. These include paroxysmal choreoathetosis with spasticity (dystonia 9); paroxysmal exercise-induced dyskinesia and epilepsy (dystonia 18); and certain types of epilepsy. In rare cases, people with variants of GLUT1 deficiency syndrome produce abnormal red blood cells and have uncommon forms of a blood condition known as anemia, which is characterized by a shortage of red blood cells.
Frequency
GLUT1 deficiency syndrome is a rare disorder. In Scotland, the incidence of the disorder has been estimated at 1 in 24,000 newborns. However, researchers suggest that the disorder may be underdiagnosed, because many neurological disorders can cause similar symptoms.
Causes
GLUT1 deficiency syndrome is caused by variants (also known as mutations) in the SLC2A1 gene. This gene provides instructions for producing a protein called the glucose transporter protein type 1 (GLUT1). The GLUT1 protein is embedded in the outer membrane surrounding cells , where it transports a simple sugar called glucose into cells from the blood or from other cells for use as fuel.
, where it transports a simple sugar called glucose into cells from the blood or from other cells for use as fuel.
In the brain, the GLUT1 protein is involved in moving glucose, which is the brain's main energy source, across the blood-brain barrier. The blood-brain barrier acts as a boundary between tiny blood vessels (capillaries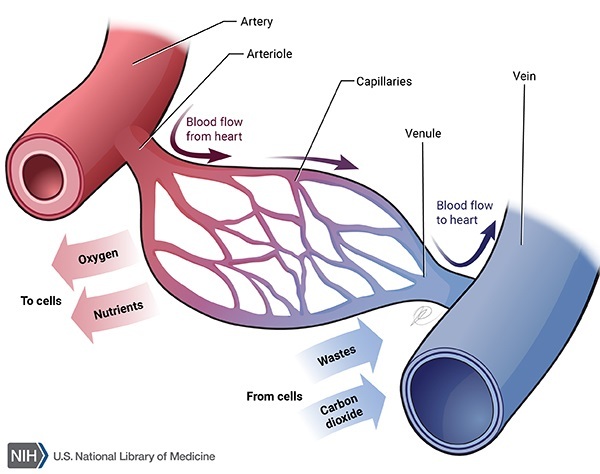 ) and the surrounding brain tissue; it protects the brain's delicate nerve tissue by preventing many other types of molecules from entering the brain. The GLUT1 protein also moves glucose between cells in the brain called glia, which protect and maintain nerve cells (neurons).
) and the surrounding brain tissue; it protects the brain's delicate nerve tissue by preventing many other types of molecules from entering the brain. The GLUT1 protein also moves glucose between cells in the brain called glia, which protect and maintain nerve cells (neurons).
SLC2A1 gene variants reduce or eliminate the function of the GLUT1 protein. Having less functional GLUT1 protein reduces the amount of glucose available to brain cells, which affects brain development and function.
Inheritance
This condition is usually inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. About 90 percent of cases of GLUT1 deficiency syndrome result from new variants in the gene. These cases occur in people with no history of the disorder in their family. In other cases, an affected person inherits the variantfrom an affected parent
in the gene. These cases occur in people with no history of the disorder in their family. In other cases, an affected person inherits the variantfrom an affected parent .
.
In a small number of families, GLUT1 deficiency syndrome is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell have variants. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell have variants. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- De Vivo disease
- Encephalopathy due to GLUT1 deficiency
- G1D
- Glucose transport defect, blood-brain barrier
- Glucose transporter protein syndrome
- Glucose transporter type 1 deficiency syndrome
- Glut1 deficiency
- GLUT1 DS
- GTPS
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Brockmann K. The expanding phenotype of GLUT1-deficiency syndrome. Brain Dev. 2009 Aug;31(7):545-52. doi: 10.1016/j.braindev.2009.02.008. Epub 2009 Mar 21. Citation on PubMed
- Klepper J, Akman C, Armeno M, Auvin S, Cervenka M, Cross HJ, De Giorgis V, Della Marina A, Engelstad K, Heussinger N, Kossoff EH, Leen WG, Leiendecker B, Monani UR, Oguni H, Neal E, Pascual JM, Pearson TS, Pons R, Scheffer IE, Veggiotti P, Willemsen M, Zuberi SM, De Vivo DC. Glut1 Deficiency Syndrome (Glut1DS): State of the art in 2020 and recommendations of the international Glut1DS study group. Epilepsia Open. 2020 Aug 13;5(3):354-365. doi: 10.1002/epi4.12414. eCollection 2020 Sep. Citation on PubMed
- Klepper J, Scheffer H, Elsaid MF, Kamsteeg EJ, Leferink M, Ben-Omran T. Autosomal recessive inheritance of GLUT1 deficiency syndrome. Neuropediatrics. 2009 Oct;40(5):207-10. doi: 10.1055/s-0030-1248264. Epub 2010 Mar 10. Citation on PubMed
- Klepper J. GLUT1 deficiency syndrome in clinical practice. Epilepsy Res. 2012 Jul;100(3):272-7. doi: 10.1016/j.eplepsyres.2011.02.007. Epub 2011 Mar 5. Citation on PubMed
- Leen WG, Klepper J, Verbeek MM, Leferink M, Hofste T, van Engelen BG, Wevers RA, Arthur T, Bahi-Buisson N, Ballhausen D, Bekhof J, van Bogaert P, Carrilho I, Chabrol B, Champion MP, Coldwell J, Clayton P, Donner E, Evangeliou A, Ebinger F, Farrell K, Forsyth RJ, de Goede CG, Gross S, Grunewald S, Holthausen H, Jayawant S, Lachlan K, Laugel V, Leppig K, Lim MJ, Mancini G, Marina AD, Martorell L, McMenamin J, Meuwissen ME, Mundy H, Nilsson NO, Panzer A, Poll-The BT, Rauscher C, Rouselle CM, Sandvig I, Scheffner T, Sheridan E, Simpson N, Sykora P, Tomlinson R, Trounce J, Webb D, Weschke B, Scheffer H, Willemsen MA. Glucose transporter-1 deficiency syndrome: the expanding clinical and genetic spectrum of a treatable disorder. Brain. 2010 Mar;133(Pt 3):655-70. doi: 10.1093/brain/awp336. Epub 2010 Feb 2. Citation on PubMed
- Leen WG, Wevers RA, Kamsteeg EJ, Scheffer H, Verbeek MM, Willemsen MA. Cerebrospinal fluid analysis in the workup of GLUT1 deficiency syndrome: a systematic review. JAMA Neurol. 2013 Nov;70(11):1440-4. doi: 10.1001/jamaneurol.2013.3090. Citation on PubMed
- Pascual JM, Wang D, Hinton V, Engelstad K, Saxena CM, Van Heertum RL, De Vivo DC. Brain glucose supply and the syndrome of infantile neuroglycopenia. Arch Neurol. 2007 Apr;64(4):507-13. doi: 10.1001/archneur.64.4.noc60165. Epub 2007 Feb 12. Citation on PubMed
- Pascual JM, Wang D, Lecumberri B, Yang H, Mao X, Yang R, De Vivo DC. GLUT1 deficiency and other glucose transporter diseases. Eur J Endocrinol. 2004 May;150(5):627-33. doi: 10.1530/eje.0.1500627. Citation on PubMed
- Pearson TS, Akman C, Hinton VJ, Engelstad K, De Vivo DC. Phenotypic spectrum of glucose transporter type 1 deficiency syndrome (Glut1 DS). Curr Neurol Neurosci Rep. 2013 Apr;13(4):342. doi: 10.1007/s11910-013-0342-7. Citation on PubMed
- Rotstein M, Engelstad K, Yang H, Wang D, Levy B, Chung WK, De Vivo DC. Glut1 deficiency: inheritance pattern determined by haploinsufficiency. Ann Neurol. 2010 Dec;68(6):955-8. doi: 10.1002/ana.22088. Citation on PubMed or Free article on PubMed Central
- Symonds JD, Zuberi SM, Stewart K, McLellan A, O'Regan M, MacLeod S, Jollands A, Joss S, Kirkpatrick M, Brunklaus A, Pilz DT, Shetty J, Dorris L, Abu-Arafeh I, Andrew J, Brink P, Callaghan M, Cruden J, Diver LA, Findlay C, Gardiner S, Grattan R, Lang B, MacDonnell J, McKnight J, Morrison CA, Nairn L, Slean MM, Stephen E, Webb A, Vincent A, Wilson M. Incidence and phenotypes of childhood-onset genetic epilepsies: a prospective population-based national cohort. Brain. 2019 Aug 1;142(8):2303-2318. doi: 10.1093/brain/awz195. Citation on PubMed or Free article on PubMed Central
- Wang D, Pascual JM, Yang H, Engelstad K, Jhung S, Sun RP, De Vivo DC. Glut-1 deficiency syndrome: clinical, genetic, and therapeutic aspects. Ann Neurol. 2005 Jan;57(1):111-8. doi: 10.1002/ana.20331. Citation on PubMed
- Wang D, Sands T, Tang M, Monani U, De Vivo D. Glucose Transporter Type 1 Deficiency Syndrome. 2002 Jul 30 [updated 2025 Mar 6]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1430/ Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.