

Description
Facioscapulohumeral muscular dystrophy is a disorder characterized by muscle weakness and wasting (atrophy). This condition gets its name from the muscles that are affected most often: those of the face (facio-), around the shoulder blades (scapulo-), and in the upper arms (humeral). The signs and symptoms of facioscapulohumeral muscular dystrophy usually appear in adolescence. However, the onset and severity of the condition varies widely. Milder cases may not become noticeable until later in life, whereas rare severe cases become apparent in infancy or early childhood.
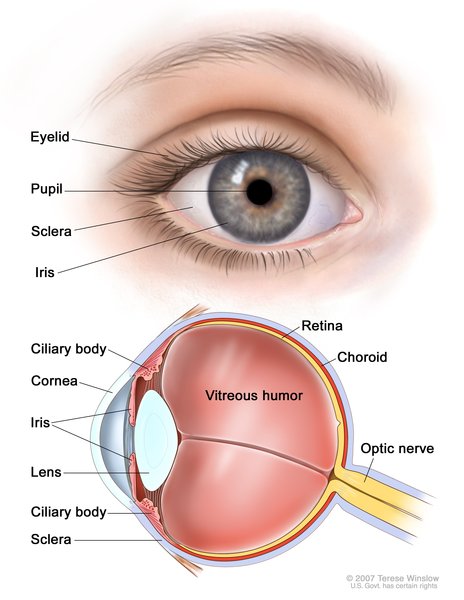
Weakness involving the facial muscles or shoulders is usually the first symptom of this condition. Facial muscle weakness often makes it difficult to drink from a straw, whistle, or turn up the corners of the mouth when smiling. Weakness in muscles around the eyes can prevent the eyes from closing fully while a person is asleep, which can lead to dry eyes and other eye problems. For reasons that are unclear, weakness may be more severe in one side of the face than the other. Weak shoulder muscles tend to make the shoulder blades (scapulae) protrude from the back, a common sign known as scapular winging. Weakness in muscles of the shoulders and upper arms can make it difficult to raise the arms over the head or throw a ball.
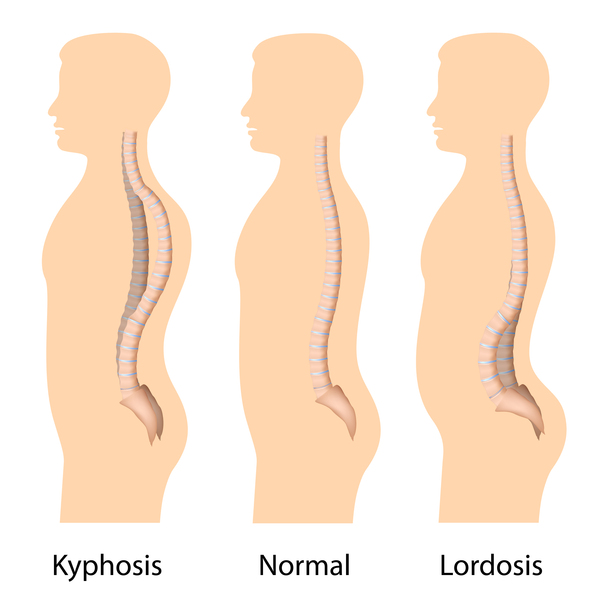
The muscle weakness associated with facioscapulohumeral muscular dystrophy worsens slowly over decades and may spread to other parts of the body. Weakness in muscles of the lower legs can lead to a condition called foot drop, which affects walking and increases the risk of falls. Muscular weakness in the hips and pelvis can make it difficult to climb stairs or walk long distances. Additionally, affected individuals may have an exaggerated curvature of the lower back (lordosis) due to weak abdominal muscles. About 20 percent of affected individuals eventually require the use of a wheelchair.
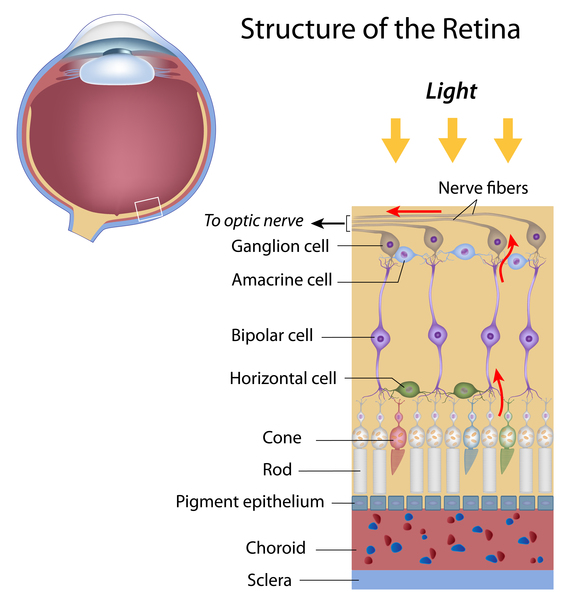
Additional signs and symptoms of facioscapulohumeral muscular dystrophy can include mild high-tone hearing loss and abnormalities involving the light-sensitive tissue at the back of the eye (the retina). These signs are often not noticeable and may be discovered only during medical testing. Rarely, facioscapulohumeral muscular dystrophy affects the heart (cardiac) muscle or muscles needed for breathing.
Researchers have described two types of facioscapulohumeral muscular dystrophy: type 1 (FSHD1) and type 2 (FSHD2). The two types have the same signs and symptoms and are distinguished by their genetic cause.
Frequency
Facioscapulohumeral muscular dystrophy has an estimated prevalence of 1 in 20,000 people. About 95 percent of all cases are FSHD1; the remaining 5 percent are FSHD2.
Causes
Facioscapulohumeral muscular dystrophy is caused by genetic changes involving the long (q) arm of chromosome 4. Both types of the disease result from changes in a region of DNA near the end of the chromosome known as D4Z4. This region consists of 11 to more than 100 repeated segments, each of which is about 3,300 DNA base pairs (3.3 kb) long. The entire D4Z4 region is normally hypermethylated, which means that it has a large number of methyl groups (consisting of one carbon atom and three hydrogen atoms) attached to the DNA. The addition of methyl groups turns off (silences) genes, so hypermethylated regions of DNA tend to have fewer genes that are turned on (active). Facioscapulohumeral muscular dystrophy results when the D4Z4 region is hypomethylated, with a shortage of attached methyl groups. In FSHD1, hypomethylation occurs because the D4Z4 region is abnormally shortened (contracted), containing between 1 and 10 repeats instead of the usual 11 to 100 repeats. In FSHD2, hypomethylation most often results from mutations in a gene called SMCHD1, which provides instructions for making a protein that normally hypermethylates the D4Z4 region. However, about 20 percent of people with FSHD2 do not have an identified mutation in the SMCHD1 gene, and the cause of the hypomethylation is unknown.
Hypermethylation of the D4Z4 region normally keeps a gene called DUX4 silenced in most adult cells and tissues. The DUX4 gene is located in the segment of the D4Z4 region closest to the end of chromosome 4. In people with facioscapulohumeral muscular dystrophy, hypomethylation of the D4Z4 region prevents the DUX4 gene from being silenced in cells and tissues where it is usually turned off. Although little is known about the function of the DUX4 gene when it is active, researchers believe that it influences the activity of other genes, particularly in muscle cells. It is unknown how abnormal activity of the DUX4 gene damages or destroys these cells, leading to progressive muscle weakness and atrophy.
The DUX4 gene is located next to a regulatory region of DNA on chromosome 4 known as a pLAM sequence, which is necessary for the production of the DUX4 protein. Some copies of chromosome 4 have a functional pLAM sequence, while others do not. Copies of chromosome 4 with a functional pLAM sequence are described as 4qA or "permissive." Those without a functional pLAM sequence are described as 4qB or "non-permissive." Without a functional pLAM sequence, no DUX4 protein is made. Because there are two copies of chromosome 4 in each cell, individuals may have two "permissive" copies of chromosome 4, two "non-permissive" copies, or one of each. Facioscapulohumeral muscular dystrophy can only occur in people who have at least one "permissive" copy of chromosome 4. Whether an affected individual has a contracted D4Z4 region or a SMCHD1 gene mutation, the disease results only if a functional pLAM sequence is also present to allow DUX4 protein to be produced.
Studies suggest that mutations in the SMCHD1 gene, which cause FSHD2, can also increase the severity of the disease in people with FSHD1. Researchers suspect that the combination of a contracted D4Z4 region and a SMCHD1 gene mutation causes the D4Z4 region to have even fewer methyl groups attached, which allows the DUX4 gene to be highly active. In people with both genetic changes, the overactive gene leads to severe muscle weakness and atrophy.
Inheritance
FSHD1 is inherited in an autosomal dominant pattern, which means one copy of the shortened D4Z4 region on a "permissive" chromosome 4 is sufficient to cause the disorder. In most cases, an affected person inherits the altered chromosome from one affected parent. Other people with FSHD1 have no history of the disorder in their family. These cases are described as sporadic and are caused by a new (de novo) D4Z4 contraction on one copy of a "permissive" chromosome 4.


FSHD2 is inherited in a digenic pattern, which means that two independent genetic changes are necessary to cause the disorder. To have FSHD2, an individual must inherit a mutation in the SMCHD1 gene (which is located on chromosome 18) and, separately, they must inherit one copy of a "permissive" chromosome 4. Affected individuals typically inherit the SMCHD1 gene mutation from one parent and the "permissive" chromosome 4 from the other parent. (Because neither parent has both genetic changes in most cases, they are typically unaffected.)
Other Names for This Condition
- Facio-scapulo-humeral dystrophy
- Facioscapulohumeral atrophy
- Facioscapulohumeral type progressive muscular dystrophy
- Facioscapuloperoneal muscular dystrophy
- FSH muscular dystrophy
- FSHD
- Muscular dystrophy, facioscapulohumeral
Additional Information & Resources
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- de Greef JC, Lemmers RJ, Camano P, Day JW, Sacconi S, Dunand M, van Engelen BG, Kiuru-Enari S, Padberg GW, Rosa AL, Desnuelle C, Spuler S, Tarnopolsky M, Venance SL, Frants RR, van der Maarel SM, Tawil R. Clinical features of facioscapulohumeral muscular dystrophy 2. Neurology. 2010 Oct 26;75(17):1548-54. doi: 10.1212/WNL.0b013e3181f96175. Citation on PubMed or Free article on PubMed Central
- Lemmers RJ, O'Shea S, Padberg GW, Lunt PW, van der Maarel SM. Best practice guidelines on genetic diagnostics of Facioscapulohumeral muscular dystrophy: workshop 9th June 2010, LUMC, Leiden, The Netherlands. Neuromuscul Disord. 2012 May;22(5):463-70. doi: 10.1016/j.nmd.2011.09.004. Epub 2011 Dec 16. No abstract available. Citation on PubMed
- Lemmers RJ, Tawil R, Petek LM, Balog J, Block GJ, Santen GW, Amell AM, van der Vliet PJ, Almomani R, Straasheijm KR, Krom YD, Klooster R, Sun Y, den Dunnen JT, Helmer Q, Donlin-Smith CM, Padberg GW, van Engelen BG, de Greef JC, Aartsma-Rus AM, Frants RR, de Visser M, Desnuelle C, Sacconi S, Filippova GN, Bakker B, Bamshad MJ, Tapscott SJ, Miller DG, van der Maarel SM. Digenic inheritance of an SMCHD1 mutation and an FSHD-permissive D4Z4 allele causes facioscapulohumeral muscular dystrophy type 2. Nat Genet. 2012 Dec;44(12):1370-4. doi: 10.1038/ng.2454. Epub 2012 Nov 11. Citation on PubMed or Free article on PubMed Central
- Lemmers RJ, van der Vliet PJ, Klooster R, Sacconi S, Camano P, Dauwerse JG, Snider L, Straasheijm KR, van Ommen GJ, Padberg GW, Miller DG, Tapscott SJ, Tawil R, Frants RR, van der Maarel SM. A unifying genetic model for facioscapulohumeral muscular dystrophy. Science. 2010 Sep 24;329(5999):1650-3. doi: 10.1126/science.1189044. Epub 2010 Aug 19. Citation on PubMed or Free article on PubMed Central
- Preston MK, Wang LH. Facioscapulohumeral Muscular Dystrophy. 1999 Mar 8 [updated 2025 Jul 10]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1443/ Citation on PubMed
- Sacconi S, Lemmers RJ, Balog J, van der Vliet PJ, Lahaut P, van Nieuwenhuizen MP, Straasheijm KR, Debipersad RD, Vos-Versteeg M, Salviati L, Casarin A, Pegoraro E, Tawil R, Bakker E, Tapscott SJ, Desnuelle C, van der Maarel SM. The FSHD2 gene SMCHD1 is a modifier of disease severity in families affected by FSHD1. Am J Hum Genet. 2013 Oct 3;93(4):744-51. doi: 10.1016/j.ajhg.2013.08.004. Epub 2013 Sep 26. Citation on PubMed or Free article on PubMed Central
- Sacconi S, Salviati L, Desnuelle C. Facioscapulohumeral muscular dystrophy. Biochim Biophys Acta. 2015 Apr;1852(4):607-14. doi: 10.1016/j.bbadis.2014.05.021. Epub 2014 May 29. Citation on PubMed
- Tawil R, van der Maarel SM, Tapscott SJ. Facioscapulohumeral dystrophy: the path to consensus on pathophysiology. Skelet Muscle. 2014 Jun 10;4:12. doi: 10.1186/2044-5040-4-12. eCollection 2014. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.