

Description
Collagen VI-related dystrophy is a group of disorders that affect skeletal muscles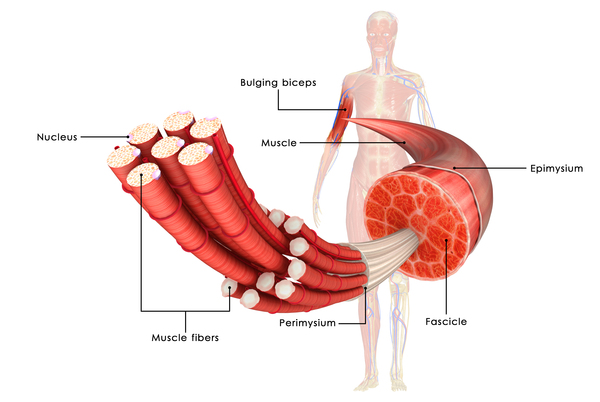 (which are the muscles used for movement) and connective tissue (which provides strength and flexibility to the skin, joints, and other structures throughout the body). Most affected individuals have muscle weakness and joint deformities called contractures that restrict movement of the affected joints and worsen over time. Researchers have described several forms of collagen VI-related dystrophy, which range in severity: Bethlem muscular dystrophy is the mildest, an intermediate form is moderate in severity, and Ullrich congenital muscular dystrophy is the most severe.
(which are the muscles used for movement) and connective tissue (which provides strength and flexibility to the skin, joints, and other structures throughout the body). Most affected individuals have muscle weakness and joint deformities called contractures that restrict movement of the affected joints and worsen over time. Researchers have described several forms of collagen VI-related dystrophy, which range in severity: Bethlem muscular dystrophy is the mildest, an intermediate form is moderate in severity, and Ullrich congenital muscular dystrophy is the most severe.
People with Bethlem muscular dystrophy usually have low muscle tone (hypotonia) in infancy. Muscle weakness can begin at any age but often appears in childhood to early adulthood. The muscle weakness is slowly progressive, with about two-thirds of affected individuals over age 50 needing walking assistance, particularly when outdoors. Affected individuals usually develop contractures by adulthood, typically in their fingers, elbows, shoulders, and ankles. Older individuals may develop weakness in respiratory muscles, which can cause breathing problems. Some people with this mild form of collagen VI-related dystrophy have skin abnormalities, including small bumps called follicular hyperkeratosis on the arms and legs; soft, velvety skin on the palms of the hands and soles of the feet; and abnormal wound healing that creates shallow scars.
The intermediate form of collagen VI-related dystrophy is characterized by muscle weakness that begins in infancy. Affected children are able to walk, although walking becomes increasingly difficult starting in early adulthood. They develop contractures in their fingers, elbows, shoulders, and ankles in childhood. In some affected people, the respiratory muscles are weakened, requiring people to use a machine to help them breathe (mechanical ventilation), particularly during sleep.
People with Ullrich congenital muscular dystrophy have severe muscle weakness beginning soon after birth. Some affected individuals are never able to walk and others can walk only with support. Those who can walk often lose the ability, usually in early adolescence. Individuals with Ullrich congenital muscular dystrophy develop contractures in their shoulders, elbows, hips, and knees, which further impair movement. Many individuals with this form of the condition have loose joints (joint laxity) in the fingers, wrists, toes, ankles, and other joints. Affected individuals need continuous mechanical ventilation to help them breathe while sleeping, and some may need it in the daytime. As in Bethlem muscular dystrophy, some people with Ullrich congenital muscular dystrophy have follicular hyperkeratosis; soft, velvety skin on the palms and soles; and abnormal wound healing.
Individuals with collagen VI-related dystrophy often have signs and symptoms of multiple forms of this condition, so it can be difficult to assign a specific diagnosis. The overlap in disease features, in addition to their common cause, is why these once separate conditions are now considered part of the same disease spectrum.
Frequency
Collagen VI-related dystrophy is rare. Bethlem muscular dystrophy is estimated to occur in 0.77 per 100,000 individuals, and Ullrich congenital muscular dystrophy is estimated to occur in 0.13 per 100,000 individuals. Only a few cases of the intermediate form have been described in the scientific literature.
Causes
Variants (also known as mutations) in the COL6A1, COL6A2, and COL6A3 genes can cause the various forms of collagen VI-related dystrophy. These genes each provide instructions for making one component of a protein called type VI collagen. Type VI collagen makes up part of the extracellular matrix that surrounds muscle cells and connective tissue. This matrix is an intricate lattice that forms in the space between cells and provides structural support. The extracellular matrix is necessary for cell stability and growth. Research suggests that type VI collagen helps secure and organize the extracellular matrix by linking the matrix to the cells it surrounds.
Variants in the COL6A1, COL6A2, and COL6A3 genes result in a decrease or lack of type VI collagen or the production of abnormal type VI collagen. While it is difficult to predict which type of variant will lead to which form of collagen VI-related dystrophy, in general, lower amounts of type VI collagen lead to more severe signs and symptoms that begin earlier in life.
Changes in type VI collagen structure or production lead to an unstable extracellular matrix that is no longer attached to cells. As a result, the stability of the surrounding muscle cells and connective tissue progressively declines, which leads to the muscle weakness, contractures, and other signs and symptoms of collagen VI-related dystrophy.
Inheritance
Collagen VI-related dystrophy is often inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. Bethlem muscular dystrophy is typically inherited in an autosomal dominant manner. The affected person usually inherits the variant from one affected parent . The intermediate form and Ullrich congenital muscular dystrophy can also follow an autosomal dominant inheritance pattern. These forms typically result from new variants
. The intermediate form and Ullrich congenital muscular dystrophy can also follow an autosomal dominant inheritance pattern. These forms typically result from new variants in the gene and occur in people with no history of the disorder in their family.
in the gene and occur in people with no history of the disorder in their family.
Less commonly, collagen VI-related dystrophy is inherited in an autosomal recessive pattern , which means both copies of the gene in each cell have variants. Some cases of Ullrich congenital muscular dystrophy and the intermediate form and a few rare instances of Bethlem muscular dystrophy are inherited in an autosomal recessive manner. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
, which means both copies of the gene in each cell have variants. Some cases of Ullrich congenital muscular dystrophy and the intermediate form and a few rare instances of Bethlem muscular dystrophy are inherited in an autosomal recessive manner. The parents of an individual with an autosomal recessive condition each carry one copy of the altered gene, but they typically do not show signs and symptoms of the condition.
Other Names for This Condition
- Col6-RDs
- Collagen type VI-related disorders
- Collagen VI-related dystrophies
- Collagen VI-related myopathies
- Collagen VI-related myopathy
- ColVI myopathies
Additional Information & Resources
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Allamand V, Brinas L, Richard P, Stojkovic T, Quijano-Roy S, Bonne G. ColVI myopathies: where do we stand, where do we go? Skelet Muscle. 2011 Sep 23;1:30. doi: 10.1186/2044-5040-1-30. Citation on PubMed or Free article on PubMed Central
- Bonnemann CG. The collagen VI-related myopathies: muscle meets its matrix. Nat Rev Neurol. 2011 Jun 21;7(7):379-90. doi: 10.1038/nrneurol.2011.81. Citation on PubMed
- Bushby KM, Collins J, Hicks D. Collagen type VI myopathies. Adv Exp Med Biol. 2014;802:185-99. doi: 10.1007/978-94-007-7893-1_12. Citation on PubMed
- Foley AR, Mohassel P, Donkervoort S, Bolduc V, Bonnemann CG. Collagen VI-Related Dystrophies. 2004 Jun 25 [updated 2021 Mar 11]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1503/ Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.