

Description
Caudal regression syndrome is a disorder that impacts the development of the lower (caudal) part of the spine. The condition can affect many parts of the lower body, including the lower back and limbs, the genitourinary tract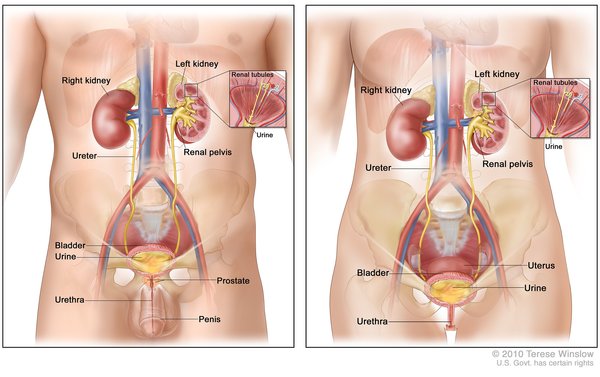 , and the gastrointestinal tract
, and the gastrointestinal tract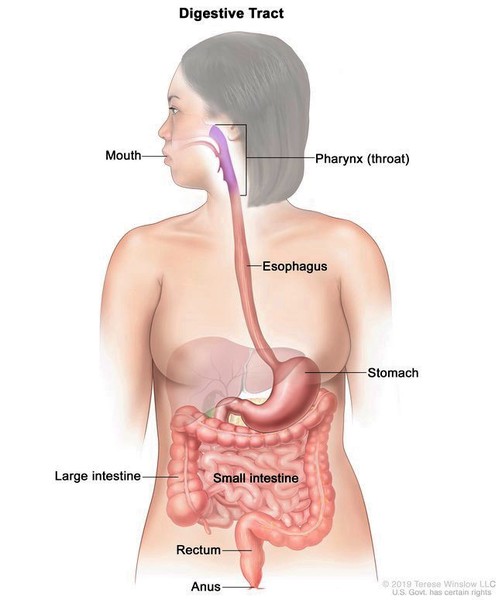 .
.
In people with this disorder, the bones of the lower spine (vertebrae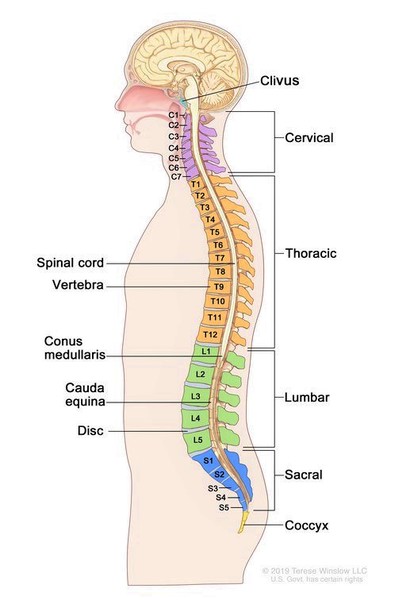 ) are misshapen or missing. The end of the spinal cord, the bundle of nerves and cells protected by the vertebrae, may also be malformed or missing. Sometimes, the spinal cord is abnormally connected (tethered) to nearby tissues. People with caudal regression syndrome can also have an abnormal curvature of the spine (lordosis or kyphosis
) are misshapen or missing. The end of the spinal cord, the bundle of nerves and cells protected by the vertebrae, may also be malformed or missing. Sometimes, the spinal cord is abnormally connected (tethered) to nearby tissues. People with caudal regression syndrome can also have an abnormal curvature of the spine (lordosis or kyphosis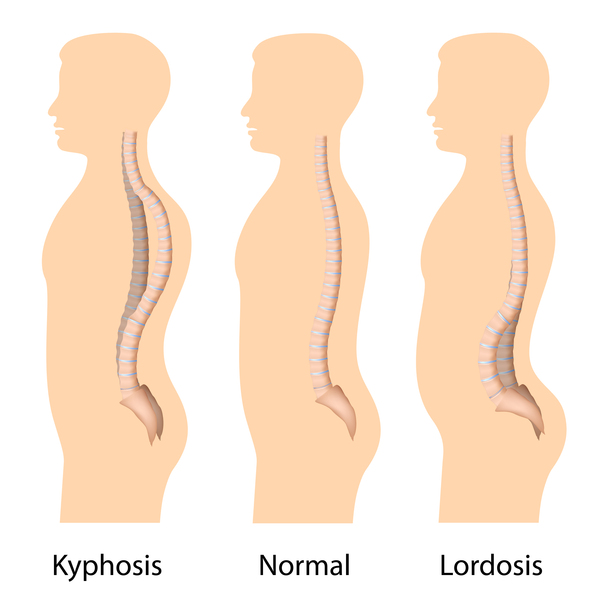 ). The spinal abnormalities may affect the size and shape of the chest, which very rarely leads to breathing problems.
). The spinal abnormalities may affect the size and shape of the chest, which very rarely leads to breathing problems.
Individuals with caudal regression syndrome may have small hip bones. The buttocks tend to be flat and dimpled. The bones of the legs are typically underdeveloped, and the joints in the lower limbs may be unusually stiff and difficult to move. In some affected individuals, the legs are bent with the knees pointing out to the side and the feet tucked underneath the hips (sometimes called a frog leg-like position). These individuals may have webbed skin behind their knees. In other affected individuals, the knees may not bend, and the legs remain in a straight position. Their feet may be inward- and upward-turning (clubfeet ) or outward- and upward-turning (calcaneovalgus). Some people with caudal regression syndrome have reduced or excessive sensation in their lower limbs. Sensitivity differs from person to person and from one area of the limb to another.
) or outward- and upward-turning (calcaneovalgus). Some people with caudal regression syndrome have reduced or excessive sensation in their lower limbs. Sensitivity differs from person to person and from one area of the limb to another.
Mobility in people with caudal regression syndrome is varied. Some individuals with the condition walk independently, and others require mobility aids, such as braces, crutches, walkers, or wheelchairs.
Abnormalities in the genitourinary tract in people with caudal regression syndrome are diverse. Urinary tract problems can result from abnormalities in the lowest part of the spinal cord, which contains the nerves that control bladder function. Damage to these nerves can cause a condition called neurogenic bladder, which makes it difficult to control the flow of urine. In addition, the kidneys may be malformed in people with caudal regression syndrome; defects include a missing kidney (unilateral renal agenesis), kidneys that are fused together (horseshoe kidney), or duplication of the tubes that carry urine from each kidney to the bladder (ureteral duplication). These kidney abnormalities and neurogenic bladder can lead to frequent urinary tract infections and the backflow (reflux) of urine into the kidneys, which damage the kidneys and can cause progressive kidney failure.
may be malformed in people with caudal regression syndrome; defects include a missing kidney (unilateral renal agenesis), kidneys that are fused together (horseshoe kidney), or duplication of the tubes that carry urine from each kidney to the bladder (ureteral duplication). These kidney abnormalities and neurogenic bladder can lead to frequent urinary tract infections and the backflow (reflux) of urine into the kidneys, which damage the kidneys and can cause progressive kidney failure.
Genital abnormalities in people with caudal regression syndrome can include the urethra opening on the underside of the penis (hypospadias) or undescended testes (cryptorchidism). Some affected people may have an abnormal connection between the rectum and vagina (rectovaginal fistula). In severe cases, people with this condition may have underdeveloped genitalia (genital agenesis).
People with caudal regression syndrome may have abnormal twisting (malrotation) of the large intestine, an obstruction of the anal opening (imperforate anus), soft out-pouchings in the lower abdomen (inguinal hernias ), or other malformations of the gastrointestinal tract. Affected individuals are often constipated and may have difficulty with bowel control.
), or other malformations of the gastrointestinal tract. Affected individuals are often constipated and may have difficulty with bowel control.
The upper part of the body can also be affected. Some people with caudal regression syndrome have a heart condition or hearing problems.
Frequency
The frequency of caudal regression syndrome is unknown. It is estimated to occur in 1 to 2.5 in 100,000 newborns. This condition is much more common among infants whose parent has diabetes while pregnant, affecting an estimated 1 in 350 newborns in this group.
Causes
Caudal regression syndrome is a complex condition that may have different causes in different people. The condition is likely caused by the interaction of multiple genetic and environmental factors. One risk factor for the development of caudal regression syndrome is the presence of diabetes during pregnancy. It is thought that increased blood sugar (glucose) levels and other metabolic problems related to diabetes may have a harmful effect on a developing fetus, increasing the likelihood of developing caudal regression syndrome. The risks to the fetus are further increased if the diabetes is poorly managed. Researchers are trying to identify other factors that contribute to the development of this complex disorder.
Some researchers believe that a disruption of fetal development around day 28 of pregnancy causes caudal regression syndrome. The developmental problem is thought to affect the middle layer of embryonic tissue known as the mesoderm. Disruption of normal mesoderm development impairs normal formation of parts of the skeleton, gastrointestinal system, and genitourinary system.
Other researchers think that caudal regression syndrome is caused by the presence of an abnormal artery in the abdomen, which diverts blood flow away from the lower areas of the developing fetus. Decreased blood flow to these areas is thought to interfere with their development and lead to the signs and symptoms of caudal regression syndrome.
Some scientists believe that the abnormal development of the mesoderm reduces the blood flow, while other scientists believe that the reduced blood flow causes the abnormal mesoderm development. Many scientists think that the cause of caudal regression syndrome is a combination of abnormal mesoderm development and decreased blood flow to the caudal areas of the fetus.
Inheritance
Caudal regression syndrome occurs sporadically, which means it occurs in people with no history of the condition in their family. Multiple genetic and environmental factors likely affect the risk of developing this condition.
Other Names for This Condition
- Caudal dysgenesis syndrome
- Caudal dysplasia sequence
- Caudal regression sequence
- CRS
- Lumbo-sacral agenesis
- SA/CRS
- Sacral agenesis
- Sacral defect with anterior meningocele
Additional Information & Resources
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Boulas MM. Recognition of caudal regression syndrome. Adv Neonatal Care. 2009 Apr;9(2):61-9; quiz 70-1. doi: 10.1097/ANC.0b013e31819de44f. Citation on PubMed
- Duesterhoeft SM, Ernst LM, Siebert JR, Kapur RP. Five cases of caudal regression with an aberrant abdominal umbilical artery: Further support for a caudal regression-sirenomelia spectrum. Am J Med Genet A. 2007 Dec 15;143A(24):3175-84. doi: 10.1002/ajmg.a.32028. Citation on PubMed
- Hentschel J, Stierkorb E, Schneider G, Goedde S, Siemer S, Gortner L. Caudal regression sequence: vascular origin? J Perinatol. 2006 Jul;26(7):445-7. doi: 10.1038/sj.jp.7211534. Citation on PubMed
- Jeelani Y, Mosich GM, McComb JG. Closed neural tube defects in children with caudal regression. Childs Nerv Syst. 2013 Sep;29(9):1451-7. doi: 10.1007/s00381-013-2119-3. Epub 2013 Sep 7. Citation on PubMed
- Thottungal AD, Charles AK, Dickinson JE, Bower C. Caudal dysgenesis and sirenomelia-single centre experience suggests common pathogenic basis. Am J Med Genet A. 2010 Oct;152A(10):2578-87. doi: 10.1002/ajmg.a.33599. Citation on PubMed
- Torre M, Buffa P, Jasonni V, Cama A. Long-term urologic outcome in patients with caudal regression syndrome, compared with meningomyelocele and spinal cord lipoma. J Pediatr Surg. 2008 Mar;43(3):530-3. doi: 10.1016/j.jpedsurg.2007.10.036. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.