

Description
Campomelic dysplasia is a severe disorder that affects development of the skeleton, reproductive system, and other parts of the body. This condition is often life-threatening in the newborn period.
The term "campomelic" comes from the Greek words for "bent limb." Affected individuals are typically born with bowing of the long bones in the legs, and occasionally, bowing in the arms. Bowing can cause characteristic skin dimples to form over the curved bone, especially on the lower legs. People with campomelic dysplasia usually have short legs, dislocated hips, underdeveloped shoulder blades, 11 pairs of ribs instead of 12, bone abnormalities in the neck, and inward- and upward-turning feet (clubfeet). These skeletal abnormalities begin developing before birth and can often be seen on ultrasound. When affected individuals have features of this disorder but do not have bowed limbs, they are said to have acampomelic campomelic dysplasia.

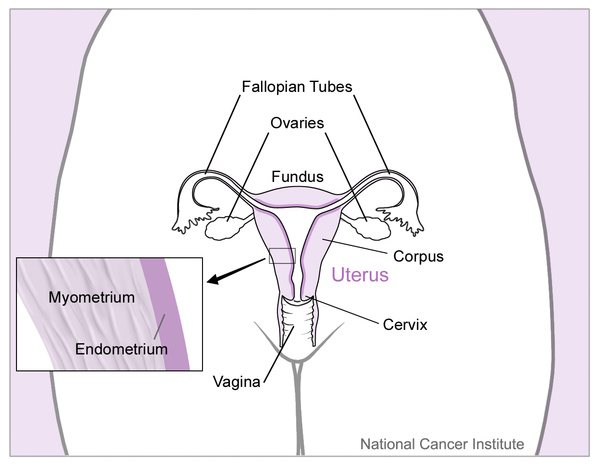
Approximately 75 percent of affected individuals with a typical male chromosome pattern (46,XY) have normal female genitalia or genitalia that do not look clearly male or clearly female. Internal reproductive organs may not correspond with the external genitalia; the internal organs can be male (testes), female (ovaries), or a combination of the two. For example, an individual with female external genitalia may have testes or a combination of testes and ovaries.
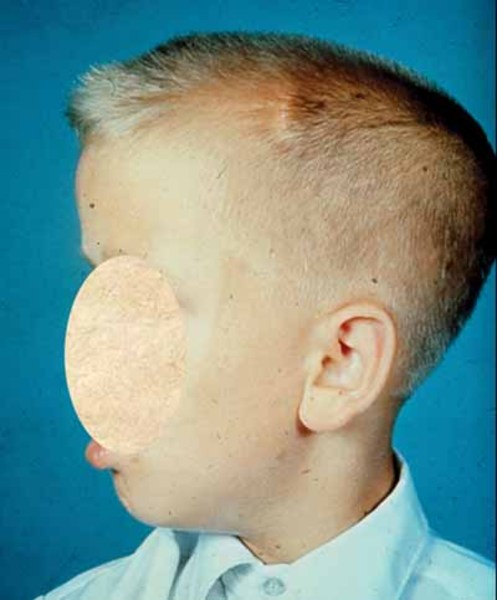
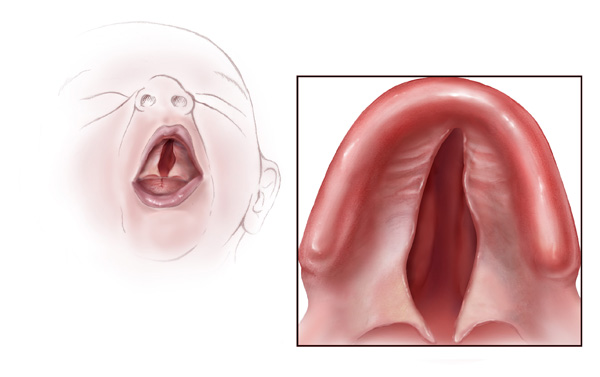
Affected individuals have distinctive facial features, including a small chin, prominent eyes, and a flat face. They also have a large head compared to their body size. A particular group of physical features, called Pierre Robin sequence, is common in people with campomelic dysplasia. Pierre Robin sequence includes an opening in the roof of the mouth (a cleft palate), a tongue that is placed further back than normal (glossoptosis), and a small lower jaw (micrognathia). People with campomelic dysplasia are often born with weakened cartilage that forms the upper respiratory tract. This abnormality, called laryngotracheomalacia, partially blocks the airway and causes difficulty breathing. Laryngotracheomalacia contributes to the poor survival of infants with campomelic dysplasia.
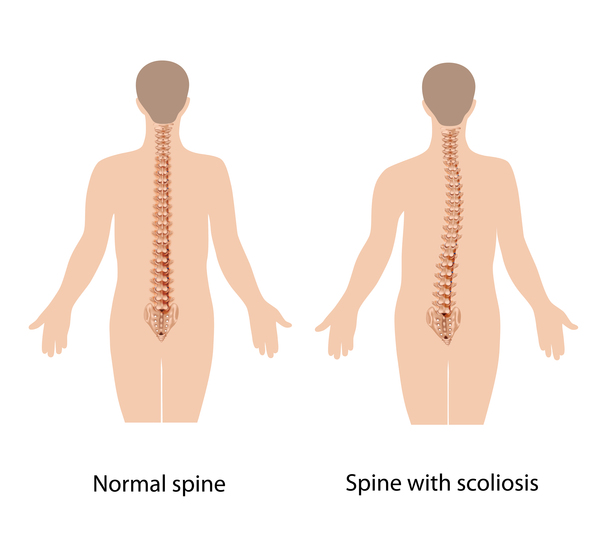
Only a few people with campomelic dysplasia survive past infancy. As these individuals age, they may develop an abnormal curvature of the spine (scoliosis) and other spine abnormalities that compress the spinal cord. People with campomelic dysplasia may also have short stature and hearing loss.
Frequency
The prevalence of campomelic dysplasia is uncertain; estimates range from 1 in 40,000 to 200,000 people.
Causes
Mutations in or near the SOX9 gene cause campomelic dysplasia. This gene provides instructions for making a protein that plays a critical role in the formation of many different tissues and organs during embryonic development. The SOX9 protein regulates the activity of other genes, especially those that are important for development of the skeleton and reproductive organs.
Most cases of campomelic dysplasia are caused by mutations within the SOX9 gene. These mutations prevent the production of the SOX9 protein or result in a protein with impaired function. About 5 percent of cases are caused by chromosome abnormalities that occur near the SOX9 gene; these cases tend to be milder than those caused by mutations within the SOX9 gene. The chromosome abnormalities disrupt regions of DNA that normally regulate the activity of the SOX9 gene. All of these genetic changes prevent the SOX9 protein from properly controlling the genes essential for normal development of the skeleton, reproductive system, and other parts of the body. Abnormal development of these structures causes the signs and symptoms of campomelic dysplasia.
Inheritance
Campomelic dysplasia is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder. Most cases result from new mutations in or near the SOX9 gene and occur in people with no history of the disorder in their family. Rarely, affected individuals inherit a chromosome abnormality from a parent who may or may not show mild signs and symptoms of campomelic dysplasia.


Other Names for This Condition
- Campomelic dwarfism
- Campomelic syndrome
- Camptomelic dysplasia
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Barone C, Bartoloni G, Baffico AM, Pappalardo E, Mura I, Ettore G, Bianca S. Novel c.358C>T mutation of SOX9 gene in prenatal diagnosis of campomelic dysplasia. Congenit Anom (Kyoto). 2014 Aug;54(3):193-4. doi: 10.1111/cga.12054. No abstract available. Citation on PubMed
- Beaulieu Bergeron M, Lemyre E, Rypens F, Scherer G, Lemieux N, Fournet JC. Diagnosis of true hermaphroditism in a fetus with acampomelic campomelic dysplasia. Prenat Diagn. 2009 May;29(5):528-30. doi: 10.1002/pd.2187. No abstract available. Citation on PubMed
- Bien-Willner GA, Stankiewicz P, Lupski JR. SOX9cre1, a cis-acting regulatory element located 1.1 Mb upstream of SOX9, mediates its enhancement through the SHH pathway. Hum Mol Genet. 2007 May 15;16(10):1143-56. doi: 10.1093/hmg/ddm061. Epub 2007 Apr 4. Citation on PubMed
- Hill-Harfe KL, Kaplan L, Stalker HJ, Zori RT, Pop R, Scherer G, Wallace MR. Fine mapping of chromosome 17 translocation breakpoints > or = 900 Kb upstream of SOX9 in acampomelic campomelic dysplasia and a mild, familial skeletal dysplasia. Am J Hum Genet. 2005 Apr;76(4):663-71. doi: 10.1086/429254. Citation on PubMed or Free article on PubMed Central
- Kobayashi A, Chang H, Chaboissier MC, Schedl A, Behringer RR. Sox9 in testis determination. Ann N Y Acad Sci. 2005 Dec;1061:9-17. doi: 10.1196/annals.1336.003. Citation on PubMed
- Leipoldt M, Erdel M, Bien-Willner GA, Smyk M, Theurl M, Yatsenko SA, Lupski JR, Lane AH, Shanske AL, Stankiewicz P, Scherer G. Two novel translocation breakpoints upstream of SOX9 define borders of the proximal and distal breakpoint cluster region in campomelic dysplasia. Clin Genet. 2007 Jan;71(1):67-75. doi: 10.1111/j.1399-0004.2007.00736.x. Citation on PubMed
- Mansour S, Offiah AC, McDowall S, Sim P, Tolmie J, Hall C. The phenotype of survivors of campomelic dysplasia. J Med Genet. 2002 Aug;39(8):597-602. doi: 10.1136/jmg.39.8.597. No abstract available. Citation on PubMed or Free article on PubMed Central
- Nelson ME, Griffin GR, Innis JW, Green GE. Campomelic dysplasia: airway management in two patients and an update on clinical-molecular correlations in the head and neck. Ann Otol Rhinol Laryngol. 2011 Oct;120(10):682-5. doi: 10.1177/000348941112001009. Citation on PubMed
- Pop R, Zaragoza MV, Gaudette M, Dohrmann U, Scherer G. A homozygous nonsense mutation in SOX9 in the dominant disorder campomelic dysplasia: a case of mitotic gene conversion. Hum Genet. 2005 Jun;117(1):43-53. doi: 10.1007/s00439-005-1295-y. Epub 2005 Apr 2. Citation on PubMed
- Smyk M, Obersztyn E, Nowakowska B, Bocian E, Cheung SW, Mazurczak T, Stankiewicz P. Recurrent SOX9 deletion campomelic dysplasia due to somatic mosaicism in the father. Am J Med Genet A. 2007 Apr 15;143A(8):866-70. doi: 10.1002/ajmg.a.31631. Citation on PubMed
- Unger S, Scherer G, Superti-Furga A. Campomelic Dysplasia. 2008 Jul 31 [updated 2023 Apr 6]. In: Adam MP, Bick S, Mirzaa GM, Pagon RA, Wallace SE, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2026. Available from http://www.ncbi.nlm.nih.gov/books/NBK1760/ Citation on PubMed
- Velagaleti GV, Bien-Willner GA, Northup JK, Lockhart LH, Hawkins JC, Jalal SM, Withers M, Lupski JR, Stankiewicz P. Position effects due to chromosome breakpoints that map approximately 900 Kb upstream and approximately 1.3 Mb downstream of SOX9 in two patients with campomelic dysplasia. Am J Hum Genet. 2005 Apr;76(4):652-62. doi: 10.1086/429252. Epub 2005 Feb 22. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.