

Description
Bartter syndrome is a group of very similar kidney disorders that cause an imbalance of potassium, sodium, chloride, and related molecules in the body.
In some cases, Bartter syndrome becomes apparent before birth. The disorder can cause polyhydramnios, which is an increased volume of fluid surrounding the fetus (amniotic fluid). Polyhydramnios increases the risk of premature birth.
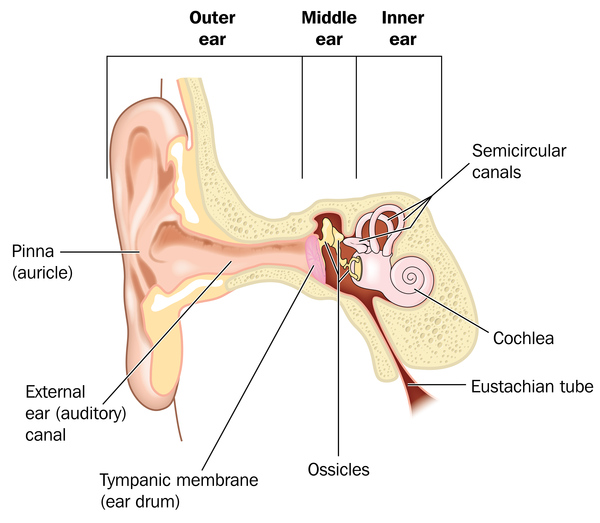
Beginning in infancy, affected individuals often fail to grow and gain weight at the expected rate (failure to thrive). They lose excess amounts of salt (sodium chloride) in their urine, which leads to dehydration, constipation, and increased urine production (polyuria). In addition, large amounts of calcium are lost through the urine (hypercalciuria), which can cause weakening of the bones (osteopenia). Some of the calcium is deposited in the kidneys as they are concentrating urine, leading to hardening of the kidney tissue (nephrocalcinosis). Bartter syndrome is also characterized by low levels of potassium in the blood (hypokalemia), which can result in muscle weakness, cramping, and fatigue. Rarely, affected children develop hearing loss caused by abnormalities in the inner ear (sensorineural deafness).
Two major forms of Bartter syndrome are distinguished by their age of onset and severity. One form begins before birth (antenatal) and is often life-threatening. The other form, often called the classical form, begins in early childhood and tends to be less severe. Once the genetic causes of Bartter syndrome were identified, researchers also split the disorder into different types based on the genes involved. Types I, II, and IV have the features of antenatal Bartter syndrome. Because type IV is also associated with hearing loss, it is sometimes called antenatal Bartter syndrome with sensorineural deafness. Type III usually has the features of classical Bartter syndrome.
Frequency
The exact prevalence of this disorder is unknown, although it likely affects about 1 per million people worldwide. The condition appears to be more common in Costa Rica and Kuwait than in other populations.
Causes
Bartter syndrome can be caused by mutations in at least five genes. Mutations in the SLC12A1 gene cause type I. Type II results from mutations in the KCNJ1 gene. Mutations in the CLCNKB gene are responsible for type III. Type IV can result from mutations in the BSND gene or from a combination of mutations in the CLCNKA and CLCNKB genes.
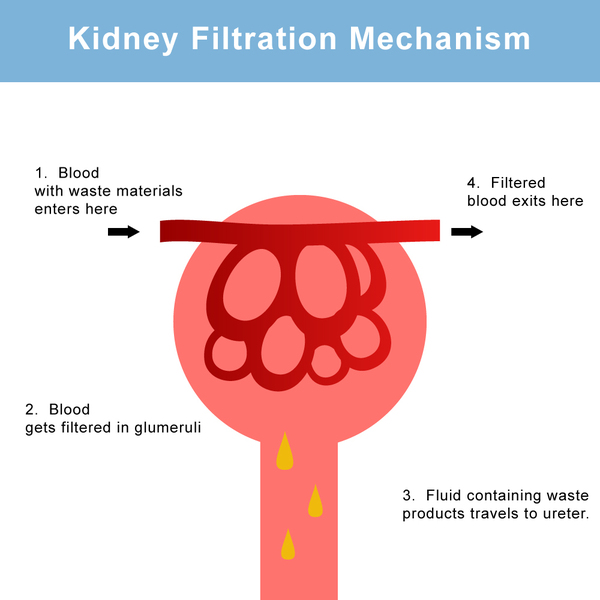
The genes associated with Bartter syndrome play important roles in normal kidney function. The proteins produced from these genes are involved in the kidneys' reabsorption of salt. Mutations in any of the five genes impair the kidneys' ability to reabsorb salt, leading to the loss of excess salt in the urine (salt wasting). Abnormalities of salt transport also affect the reabsorption of other charged atoms (ions), including potassium and calcium. The resulting imbalance of ions in the body leads to the major features of Bartter syndrome.
In some people with Bartter syndrome, the genetic cause of the disorder is unknown. Researchers are searching for additional genes that may be associated with this condition.
Inheritance
This condition is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.

Other Names for This Condition
- Aldosteronism with hyperplasia of the adrenal cortex
- Bartter disease
- Bartter's syndrome
- Juxtaglomerular hyperplasia with secondary aldosteronism
Additional Information & Resources
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Hebert SC. Bartter syndrome. Curr Opin Nephrol Hypertens. 2003 Sep;12(5):527-32. doi: 10.1097/00041552-200309000-00008. Citation on PubMed
- Kleta R, Bockenhauer D. Bartter syndromes and other salt-losing tubulopathies. Nephron Physiol. 2006;104(2):p73-80. doi: 10.1159/000094001. Epub 2006 Jun 19. Citation on PubMed
- Proesmans W. Threading through the mizmaze of Bartter syndrome. Pediatr Nephrol. 2006 Jul;21(7):896-902. doi: 10.1007/s00467-006-0113-7. Epub 2006 May 16. Citation on PubMed
- Seyberth HW. An improved terminology and classification of Bartter-like syndromes. Nat Clin Pract Nephrol. 2008 Oct;4(10):560-7. doi: 10.1038/ncpneph0912. Epub 2008 Aug 12. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.