

Description
Gout is a type of arthritis, which is a group of related disorders caused by episodes of abnormal inflammation in the joints. People with gout have high levels of a substance called urate in the blood (hyperuricemia). Gout develops when hyperuricemia leads to the formation of urate crystals in joints, triggering an inflammatory response from the immune system.

In people with gout, the first episode of inflammation (called a flare) usually affects the big toe or other joints in the foot or ankle. If urate levels remain high, flares can recur, affecting additional joints throughout the body. The time between flares varies among affected individuals; however, most people who experience multiple flares have their second one within a year of their first.
Flares usually begin at night and can last several days. It is unclear what causes a flare to stop; the body likely turns off the inflammation response after a certain period of time. During a flare, individuals can experience throbbing or burning pain, swelling, warmth, redness, and difficulty moving the affected joint. Fevers may occur, after which the skin over the affected joint can begin to peel. Without treatment, people with gout can experience frequent flares and joint pain and damage, which can limit mobility and decrease quality of life.
In about 15 percent of people with gout, urate accumulates in the kidneys and forms kidney stones. As the condition worsens, urate crystals can also be deposited under the skin or in other soft tissue, forming a nodule called a tophus (plural: tophi). These tophi often form in the hands, elbows, or feet. Tophi do not typically cause pain, but they can become inflamed, infected, or ooze fluid. Depending on their location, tophi can interfere with movements such as walking or gripping objects.
Many people with gout also have other health conditions. Most affected individuals have high blood pressure (hypertension), chronic kidney disease, or obesity. Some also have diabetes, heart disease, or a history of stroke. It is unclear whether gout is the cause of a person's increased risk for these conditions, or whether the conditions cause the development of gout, or whether both of these situations occur to influence disease.
Frequency
Gout is a common condition, but it occurs more frequently in some populations than others. For example, gout occurs in 1 percent of people with Asian ancestry, 3 to 4 percent of people with European ancestry, and 6 to 8 percent of Indigenous (native) Taiwanese peoples and Māori from New Zealand.
Causes
Gout is caused by a combination of genetic and environmental factors. Some of the factors that contribute to this condition have been confirmed by research, while others are unknown. The main risk factor for developing gout is hyperuricemia. About one-quarter of individuals with hyperuricemia go on to develop gout. It is unclear why others with hyperuricemia do not get gout.
Large studies have identified dozens of genes that play a role in the development of gout. Multiple genetic changes, each with a small effect, likely combine to increase the risk of developing this disorder. Most of the known genes play a role in transporting urate, which is a byproduct of normal biochemical processes. Many gout-associated genes play a role in releasing urate into the urine if levels are too high or reabsorbing it back into the bloodstream if more is needed in the body. Other associated genes are involved in transporting or breaking down sugars or transporting other small molecules. The roles of some associated genes are unclear. Of all the genes that have been studied, two genes, SLC2A9 and ABCG2, seem to have the greatest influence on urate levels.
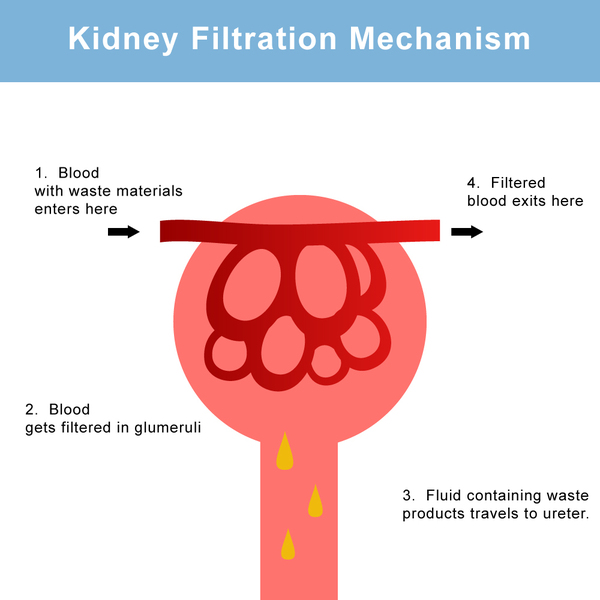
The SLC2A9 gene provides instructions for making a protein that is found primarily in the kidneys where it plays a role in managing the body's levels of urate. This protein helps reabsorb urate into the bloodstream or release it into the urine. Genetic changes in the SLC2A9 gene that can result in hyperuricemia increase the reabsorption of urate into the bloodstream and decrease its release into the urine.
The ABCG2 gene provides instructions for making a protein that helps release urate into the gut so that it can be removed from the body. Genetic changes in the ABCG2 gene that can result in hyperuricemia reduce the protein's ability to release urate into the gut.
Nongenetic factors are also believed to play a role in gout, primarily by triggering flares. These factors also often increase urate levels in the body. Consuming foods and beverages that are high in molecules called purines, such as red meat, seafood, dried beans, alcohol, and sugar-sweetened beverages can lead to increased urate. When purines are broken down, urate is made, which can cause hyperuricemia and lead to gout in some individuals. The risk for gout also increases with age. In particular, women have an increased risk after menopause. Following menopause, production of the hormone estrogen, which plays a role in removing urate from the body, declines so older women have a rise in urate levels and an increased risk of developing gout.
Inheritance
The inheritance pattern of gout is unclear because many genetic and environmental factors appear to be involved. However, having a close relative with gout likely increases a person's risk of developing the condition.
Other Names for This Condition
- Arthritis, gouty
- Articular gout
- Gouty arthritis
- Gouty arthropathy
Additional Information & Resources
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet. 2016 Oct 22;388(10055):2039-2052. doi: 10.1016/S0140-6736(16)00346-9. Epub 2016 Apr 21. Citation on PubMed
- Dalbeth N, Stamp LK, Merriman TR. The genetics of gout: towards personalised medicine? BMC Med. 2017 May 31;15(1):108. doi: 10.1186/s12916-017-0878-5. Citation on PubMed or Free article on PubMed Central
- Ichida K, Matsuo H, Takada T, Nakayama A, Murakami K, Shimizu T, Yamanashi Y, Kasuga H, Nakashima H, Nakamura T, Takada Y, Kawamura Y, Inoue H, Okada C, Utsumi Y, Ikebuchi Y, Ito K, Nakamura M, Shinohara Y, Hosoyamada M, Sakurai Y, Shinomiya N, Hosoya T, Suzuki H. Decreased extra-renal urate excretion is a common cause of hyperuricemia. Nat Commun. 2012 Apr 3;3:764. doi: 10.1038/ncomms1756. Citation on PubMed or Free article on PubMed Central
- Khanna D, Fitzgerald JD, Khanna PP, Bae S, Singh MK, Neogi T, Pillinger MH, Merill J, Lee S, Prakash S, Kaldas M, Gogia M, Perez-Ruiz F, Taylor W, Liote F, Choi H, Singh JA, Dalbeth N, Kaplan S, Niyyar V, Jones D, Yarows SA, Roessler B, Kerr G, King C, Levy G, Furst DE, Edwards NL, Mandell B, Schumacher HR, Robbins M, Wenger N, Terkeltaub R; American College of Rheumatology. 2012 American College of Rheumatology guidelines for management of gout. Part 1: systematic nonpharmacologic and pharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res (Hoboken). 2012 Oct;64(10):1431-46. doi: 10.1002/acr.21772. No abstract available. Citation on PubMed or Free article on PubMed Central
- Khanna D, Khanna PP, Fitzgerald JD, Singh MK, Bae S, Neogi T, Pillinger MH, Merill J, Lee S, Prakash S, Kaldas M, Gogia M, Perez-Ruiz F, Taylor W, Liote F, Choi H, Singh JA, Dalbeth N, Kaplan S, Niyyar V, Jones D, Yarows SA, Roessler B, Kerr G, King C, Levy G, Furst DE, Edwards NL, Mandell B, Schumacher HR, Robbins M, Wenger N, Terkeltaub R; American College of Rheumatology. 2012 American College of Rheumatology guidelines for management of gout. Part 2: therapy and antiinflammatory prophylaxis of acute gouty arthritis. Arthritis Care Res (Hoboken). 2012 Oct;64(10):1447-61. doi: 10.1002/acr.21773. No abstract available. Citation on PubMed or Free article on PubMed Central
- Kottgen A, Albrecht E, Teumer A, Vitart V, Krumsiek J, Hundertmark C, Pistis G, Ruggiero D, O'Seaghdha CM, Haller T, Yang Q, Tanaka T, Johnson AD, Kutalik Z, Smith AV, Shi J, Struchalin M, Middelberg RP, Brown MJ, Gaffo AL, Pirastu N, Li G, Hayward C, Zemunik T, Huffman J, Yengo L, Zhao JH, Demirkan A, Feitosa MF, Liu X, Malerba G, Lopez LM, van der Harst P, Li X, Kleber ME, Hicks AA, Nolte IM, Johansson A, Murgia F, Wild SH, Bakker SJ, Peden JF, Dehghan A, Steri M, Tenesa A, Lagou V, Salo P, Mangino M, Rose LM, Lehtimaki T, Woodward OM, Okada Y, Tin A, Muller C, Oldmeadow C, Putku M, Czamara D, Kraft P, Frogheri L, Thun GA, Grotevendt A, Gislason GK, Harris TB, Launer LJ, McArdle P, Shuldiner AR, Boerwinkle E, Coresh J, Schmidt H, Schallert M, Martin NG, Montgomery GW, Kubo M, Nakamura Y, Tanaka T, Munroe PB, Samani NJ, Jacobs DR Jr, Liu K, D'Adamo P, Ulivi S, Rotter JI, Psaty BM, Vollenweider P, Waeber G, Campbell S, Devuyst O, Navarro P, Kolcic I, Hastie N, Balkau B, Froguel P, Esko T, Salumets A, Khaw KT, Langenberg C, Wareham NJ, Isaacs A, Kraja A, Zhang Q, Wild PS, Scott RJ, Holliday EG, Org E, Viigimaa M, Bandinelli S, Metter JE, Lupo A, Trabetti E, Sorice R, Doring A, Lattka E, Strauch K, Theis F, Waldenberger M, Wichmann HE, Davies G, Gow AJ, Bruinenberg M; LifeLines Cohort Study; Stolk RP, Kooner JS, Zhang W, Winkelmann BR, Boehm BO, Lucae S, Penninx BW, Smit JH, Curhan G, Mudgal P, Plenge RM, Portas L, Persico I, Kirin M, Wilson JF, Mateo Leach I, van Gilst WH, Goel A, Ongen H, Hofman A, Rivadeneira F, Uitterlinden AG, Imboden M, von Eckardstein A, Cucca F, Nagaraja R, Piras MG, Nauck M, Schurmann C, Budde K, Ernst F, Farrington SM, Theodoratou E, Prokopenko I, Stumvoll M, Jula A, Perola M, Salomaa V, Shin SY, Spector TD, Sala C, Ridker PM, Kahonen M, Viikari J, Hengstenberg C, Nelson CP; CARDIoGRAM Consortium; DIAGRAM Consortium; ICBP Consortium; MAGIC Consortium; Meschia JF, Nalls MA, Sharma P, Singleton AB, Kamatani N, Zeller T, Burnier M, Attia J, Laan M, Klopp N, Hillege HL, Kloiber S, Choi H, Pirastu M, Tore S, Probst-Hensch NM, Volzke H, Gudnason V, Parsa A, Schmidt R, Whitfield JB, Fornage M, Gasparini P, Siscovick DS, Polasek O, Campbell H, Rudan I, Bouatia-Naji N, Metspalu A, Loos RJ, van Duijn CM, Borecki IB, Ferrucci L, Gambaro G, Deary IJ, Wolffenbuttel BH, Chambers JC, Marz W, Pramstaller PP, Snieder H, Gyllensten U, Wright AF, Navis G, Watkins H, Witteman JC, Sanna S, Schipf S, Dunlop MG, Tonjes A, Ripatti S, Soranzo N, Toniolo D, Chasman DI, Raitakari O, Kao WH, Ciullo M, Fox CS, Caulfield M, Bochud M, Gieger C. Genome-wide association analyses identify 18 new loci associated with serum urate concentrations. Nat Genet. 2013 Feb;45(2):145-54. doi: 10.1038/ng.2500. Epub 2012 Dec 23. Citation on PubMed or Free article on PubMed Central
- Merriman T. Genomic Influences on Hyperuricemia and Gout. Rheum Dis Clin North Am. 2017 Aug;43(3):389-399. doi: 10.1016/j.rdc.2017.04.004. Citation on PubMed
- Newberry SJ, FitzGerald JD, Motala A, Booth M, Maglione MA, Han D, Tariq A, O'Hanlon CE, Shanman R, Dudley W, Shekelle PG. Diagnosis of Gout: A Systematic Review in Support of an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2017 Jan 3;166(1):27-36. doi: 10.7326/M16-0462. Epub 2016 Nov 1. Citation on PubMed
- Richette P, Doherty M, Pascual E, Barskova V, Becce F, Castaneda-Sanabria J, Coyfish M, Guillo S, Jansen TL, Janssens H, Liote F, Mallen C, Nuki G, Perez-Ruiz F, Pimentao J, Punzi L, Pywell T, So A, Tausche AK, Uhlig T, Zavada J, Zhang W, Tubach F, Bardin T. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017 Jan;76(1):29-42. doi: 10.1136/annrheumdis-2016-209707. Epub 2016 Jul 25. Citation on PubMed
- Shekelle PG, Newberry SJ, FitzGerald JD, Motala A, O'Hanlon CE, Tariq A, Okunogbe A, Han D, Shanman R. Management of Gout: A Systematic Review in Support of an American College of Physicians Clinical Practice Guideline. Ann Intern Med. 2017 Jan 3;166(1):37-51. doi: 10.7326/M16-0461. Epub 2016 Nov 1. Citation on PubMed
- Wei WH, Guo Y, Kindt AS, Merriman TR, Semple CA, Wang K, Haley CS. Abundant local interactions in the 4p16.1 region suggest functional mechanisms underlying SLC2A9 associations with human serum uric acid. Hum Mol Genet. 2014 Oct 1;23(19):5061-8. doi: 10.1093/hmg/ddu227. Epub 2014 May 12. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.