

Description
Chronic myeloid leukemia is a slow-growing cancer of the blood-forming tissue (bone marrow). Normal bone marrow produces red blood cells (erythrocytes) that carry oxygen, white blood cells (leukocytes) that protect the body from infection, and platelets (thrombocytes) that are involved in blood clotting. In chronic myeloid leukemia, the bone marrow produces too many white blood cells. Initially, these cells function relatively normally. However, as the condition progresses, immature white blood cells called myeloblasts (or blasts) accumulate in the blood and bone marrow. The overgrowth of myeloblasts impairs development of other blood cells, leading to a shortage of red blood cells (anemia) and platelets.

Chronic myeloid leukemia usually begins after age 60. Common features include excessive tiredness (fatigue), fever, and weight loss. Many affected individuals develop an enlarged spleen (splenomegaly), which can cause a feeling of fullness in the abdomen and a loss of appetite. About half of people with chronic myeloid leukemia do not initially have any signs and symptoms and are diagnosed when a blood test is performed for another reason.
The condition consists of three phases: the chronic phase, the accelerated phase, and the blast phase (or blast crisis). In the chronic phase, the number of mature white blood cells is elevated, and myeloblasts account for less than 10 percent of blood cells. Signs and symptoms of the condition during this phase are typically mild or absent and worsen slowly. The chronic phase can last from months to years. In the accelerated phase, the number of myeloblasts is slightly higher, making up 10 to 29 percent of blood cells. The signs and symptoms continue to worsen. The accelerated phase usually lasts 4 to 6 months, although it is skipped in some affected individuals. In blast crisis, 30 percent or more of blood or bone marrow cells are myeloblasts. Signs and symptoms are most severe in this phase, including a massively enlarged spleen, bone pain, and weight loss. Serious infections and uncontrolled bleeding can be life-threatening.
Frequency
Chronic myeloid leukemia occurs in about 1 in 555 individuals. It accounts for about 10 percent of all blood cell cancers (leukemias).
Causes
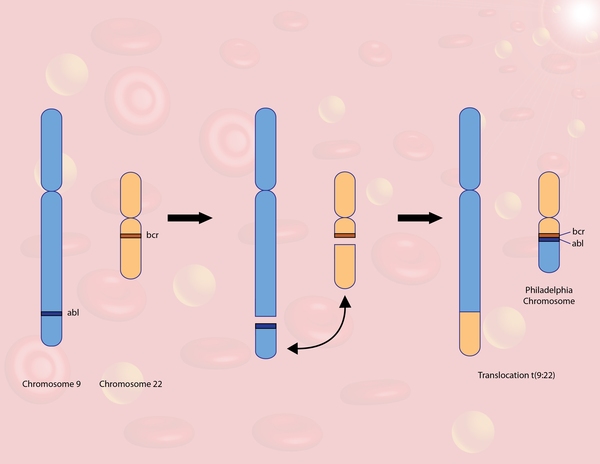
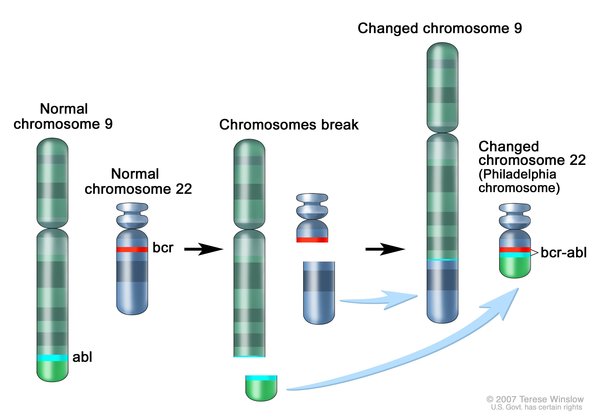
Chronic myeloid leukemia is caused by a rearrangement (translocation) of genetic material between chromosome 9 and chromosome 22. This translocation, written as t(9;22), fuses part of the ABL1 gene from chromosome 9 with part of the BCR gene from chromosome 22, creating an abnormal fusion gene called BCR-ABL1. The abnormal chromosome 22, containing a piece of chromosome 9 and the fusion gene is often referred to as the Philadelphia chromosome (named for where it was first discovered). The translocation is acquired during a person's lifetime and is present only in abnormal blood cells. This type of genetic change, called a somatic mutation, is not inherited.
The function of the protein produced from the normal BCR gene is not completely understood, although it has been shown to help control signaling in cells. The protein produced from the normal ABL1 gene is involved in many cellular processes, including cell growth and division (proliferation), maturation (differentiation), movement (migration), and self-destruction (apoptosis).
Like the ABL1 protein, the abnormal protein produced from the fusion gene, called BCR-ABL1, can promote cell proliferation and block apoptosis. However, unlike ABL1, it does not require signals in the cell to turn it on. The constantly active BCR-ABL1 protein signals cells to continue dividing abnormally and prevents them from self-destructing, which leads to overproduction of the abnormal cells and, eventually, a shortage of normal blood cells. The presence of the Philadelphia chromosome provides a target for molecular therapies in people with chronic myeloid leukemia.
In 5 to 10 percent of cases of chronic myeloid leukemia, the BCR-ABL1 fusion gene is created by complex rearrangements that involve other chromosomes in addition to chromosomes 9 and 22. These genetic changes are called variant Philadelphia translocations. These cases are similar to those caused by t(9;22).
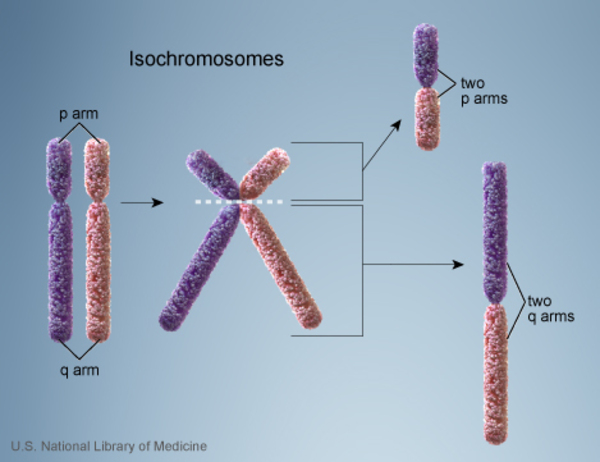
Researchers believe that additional genetic changes play a role in the progression of the chronic phase of chronic myeloid leukemia to the accelerated phase and blast crisis. The most common genetic changes associated with progression to blast crisis include an extra copy of chromosome 8 (trisomy 8), an abnormality of chromosome 17 known as isochromosome 17, and an extra copy (duplication) of the Philadelphia chromosome. When these somatic mutations occur in cells with the Philadelphia chromosome, they likely further promote uncontrolled cell proliferation.
Inheritance
This condition is generally not inherited but arises from a mutation in the body's cells that occurs after conception. This alteration is called a somatic mutation.
Other Names for This Condition
- CGL
- Chronic granulocytic leukemia
- Chronic myelocytic leukemia
- Chronic myelogenous leukemia
- CML
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Chereda B, Melo JV. Natural course and biology of CML. Ann Hematol. 2015 Apr;94 Suppl 2:S107-21. doi: 10.1007/s00277-015-2325-z. Epub 2015 Mar 27. Citation on PubMed
- Deininger MW. Diagnosing and managing advanced chronic myeloid leukemia. Am Soc Clin Oncol Educ Book. 2015:e381-8. doi: 10.14694/EdBook_AM.2015.35.e381. Citation on PubMed
- Druker BJ, Tamura S, Buchdunger E, Ohno S, Segal GM, Fanning S, Zimmermann J, Lydon NB. Effects of a selective inhibitor of the Abl tyrosine kinase on the growth of Bcr-Abl positive cells. Nat Med. 1996 May;2(5):561-6. doi: 10.1038/nm0596-561. Citation on PubMed
- Eyupoglu D, Bozkurt S, Haznedaroglu I, Buyukasik Y, Guven D. The Impact of Variant Philadelphia Chromosome Translocations on the Clinical Course of Chronic Myeloid Leukemia. Turk J Haematol. 2016 Mar 5;33(1):60-5. doi: 10.4274/tjh.2015.0237. Citation on PubMed or Free article on PubMed Central
- Lugo TG, Pendergast AM, Muller AJ, Witte ON. Tyrosine kinase activity and transformation potency of bcr-abl oncogene products. Science. 1990 Mar 2;247(4946):1079-82. doi: 10.1126/science.2408149. Citation on PubMed
- Perrotti D, Jamieson C, Goldman J, Skorski T. Chronic myeloid leukemia: mechanisms of blastic transformation. J Clin Invest. 2010 Jul;120(7):2254-64. doi: 10.1172/JCI41246. Epub 2010 Jul 1. Citation on PubMed or Free article on PubMed Central
- Quintas-Cardama A, Cortes JE. Chronic myeloid leukemia: diagnosis and treatment. Mayo Clin Proc. 2006 Jul;81(7):973-88. doi: 10.4065/81.7.973. Citation on PubMed
- Skorski T. Genetic mechanisms of chronic myeloid leukemia blastic transformation. Curr Hematol Malig Rep. 2012 Jun;7(2):87-93. doi: 10.1007/s11899-012-0114-5. Citation on PubMed
- Wang JY. The capable ABL: what is its biological function? Mol Cell Biol. 2014 Apr;34(7):1188-97. doi: 10.1128/MCB.01454-13. Epub 2014 Jan 13. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.